

Data
Systems for monitoring antibiotic resistance and antibiotic use make it possible to track trends in these major public health issues.
Recovery in hospital antibiotic use by 2022
In 2022, the monitoring of antibiotic consumption by the Spares initiative—coordinated by CPias Grand-Est and CPias Nouvelle-Aquitaine and led by Santé publique France—reports an overall consumption among participating healthcare facilities of 296 defined daily doses (DDD) per 1,000 hospital days (HD), representing a marked increase. This result covers 1,573 participating healthcare facilities (HFs), representing approximately 80% of hospital days (HD) in France.
296
defined daily doses / 1,000 hospital days
Antibiotic use varies by clinical specialty
The quantity and type of antibiotics used varied by clinical specialty.
In psychiatry, long-term care, and gynecology-obstetrics, the most commonly used antibiotics were amoxicillin, with or without clavulanic acid, whereas in intensive care, hematology, and infectious diseases, a wide variety of antibiotics was used, in line with the infectious conditions treated in these different clinical sectors. Carbapenems, glycopeptides, and daptomycin were primarily used in intensive care, internal medicine, surgery, and pediatrics.
In pediatrics, since the doses used to treat a child are lower, the exposure of hospitalized children is underestimated because, by convention, the “standard dose” used to measure antibiotic consumption is defined for a 70-kg adult (thus, one “standard dose” corresponds to several pediatric doses used).
Consumption varies depending on the antibiotic
Over the 2012–2022 period, the consumption of certain antibiotics or classes of antibiotics decreased: fluoroquinolones, glycopeptides, and the amoxicillin/clavulanic acid combination in particular, while the consumption of other antibiotics has increased: the piperacillin-tazobactam combination, third-generation cephalosporins, carbapenems, linezolid, and daptomycin.
Overall, the share of broad-spectrum antibiotics and certain antibiotics active against methicillin-resistant staphylococci in total consumption increased during the period.
rapport/synthèse
21 November 2023
Preventing Antibiotic Resistance: A "One Health" Approach - November 2023

infographie
13 November 2023
Antibiotic prescriptions in private practice: recovery confirmed in 2022

enquêtes/études
24 November 2023
Monitoring of Antibiotic Use and Bacterial Resistance in Healthcare Facilities. Spares Project. Summary Results, 2022
Antibiotic Use in Urban Areas: Encouraging Trends
What will antibiotic use in community settings in France look like in 2022?
Total antibiotic consumption in the outpatient sector is estimated at 21.6 DDD/1,000 inhabitants/day in 2022, or 821.5 prescriptions per 1,000 inhabitants per year.
Consumption varies significantly by patient age and gender. It is generally higher among women than among men. It is higher among children aged 0 to 4 and among adults aged 65 and older; it is lower among those aged 5 to 14.
The most commonly used antibiotics in 2022 are beta-lactams, including amoxicillin, which is prescribed as first-line treatment in accordance with the guidelines for the selection and duration of antibiotic therapy recommended for common bacterial infections published by the Haute Autorité de Santé and the recommendations issued by several medical societies.
What trends were observed in the private sector between 2012 and 2022?
Antibiotic use in the outpatient sector declined steadily and moderately between 2012 and 2019. In 2020, it fell sharply, mainly due to the COVID-19 pandemic, which led to a decline in routine outpatient care and, consequently, fewer prescriptions, particularly during the first lockdown. The pandemic also altered individual behaviors and contributed to stricter hygiene measures that help prevent bacterial infections.
In 2021, antibiotic consumption began to rise again: +4.9% in over-the-counter sales and +6% in prescriptions, but it remains lower than in 2019. This increase is largely due to the fact that 2021 saw much shorter lockdown periods than in 2020, as well as the return of typical seasonal infections, whose prevalence had been much lower in 2020.
Medical practices have evolved: in line with best practice recommendations, the period 2011–2021 saw a shift in the types of antibiotics prescribed, with an increase in the use of beta-lactams (broad-spectrum penicillins, including amoxicillin) and a decrease in the use of cephalosporins (antibiotics that are more likely to cause resistance).
In 2022, antibiotic consumption rose again: +14% in daily doses and +16.6% in prescriptions. However, it remains slightly lower than in 2019.
The sharp rebound in consumption in 2022 can be explained primarily by more frequent prescribing of antibiotics during consultations or visits, particularly to treat common—often winter-related—conditions. Regarding flu-like syndromes, the 2022–2023 season was marked by an exceptionally long and early epidemic, contributing to the sharp increase in consumption observed at the end of the year.
Similarly, acute gastroenteritis—which may lead to antibiotic treatment, even though it is often viral in origin—has returned to levels comparable to those before the pandemic.
1 It should be noted that while prescriptions can be compared across age groups, this is not possible for the AAD indicator. Indeed, there is no pediatric AAD, and converting children’s consumption based on “adult” AADs leads to an underestimation of their consumption.
2 Source: Santé Publique France "Preliminary Report on the 2021-2022 Flu Epidemic," published on June 1, 2022, and Acute Gastroenteritis Epidemiological Bulletin, Week 52. 2021-2022 Season.
Varied results across regions
Disparities in consumption are observed at the regional level (data available via Géodes). However, analyzing them is complex. Indeed, many factors must be taken into account to correctly interpret the observed differences. The population’s health status, life expectancy, healthcare supply, medical activity, and age distribution vary from one region to another. These factors lead to differing patterns of healthcare utilization and, consequently, varying levels of antibiotic consumption.
Between 2010 and 2019, antibiotic consumption, expressed in DDDs, remained stable or declined slightly in most regions; at the same time, the number of prescriptions decreased in almost all regions. In 2020, regardless of the indicator used, consumption declined sharply in all regions. Intra-regional trends do not differ significantly from the trend observed at the national level. In 2021 and 2022, a recovery in consumption is not observed in all regions.
Regardless of the year considered, antibiotic consumption is consistently lower in the overseas regions. In mainland France, the highest regional consumption levels are observed in Hauts-de-France, Provence-Alpes-Côte d'Azur, and Corsica.
These differences justify tailoring and adapting national initiatives promoting the appropriate use of antibiotics to each specific region.
rapport/synthèse
13 November 2023
Antibiotic Use in the Private Sector in France, 2012–2022
infographie
13 November 2023
Antibiotic prescriptions in private practice: recovery confirmed in 2022

Antibiotic Use in Nursing Homes: Initial National Data for Nursing Homes Without In-House Pharmacies
What will antibiotic use look like in 2022?
Data on residents in nursing homes without an in-house pharmacy (PUI) who are eligible for individual reimbursement by the Health Insurance system have been collected since 2021. This data covers antibiotic use and length of stay. It has enabled the production of indicators specific to residents in nursing homes without an in-house pharmacy (84% of facilities in 2015) for the period 2015–2022.
Between 2015 and 2022, antibiotic consumption in nursing homes without PUI followed a downward trend, and, as in the outpatient sector, a very sharp decrease was observed in 2020. However, unlike the outpatient sector (taken as a whole), consumption continued to decline in 2021 (-10.3% in daily doses and -9.6% in prescriptions). These divergent trends can be explained in particular by the fact that the protocols implemented in nursing homes to ensure the protection of residents were not relaxed until May and then August 2021, and all preventive measures continued to be observed, particularly the wearing of masks indoors.
In 2022, however, consumption increased. It stood at 40.5/DDJ/1,000 Jheb (+11.4% compared to 2021) and 4.07 prescriptions/1,000 Jheb (+10.5% compared to 2021). The gradual return to protocols similar to those in effect before the pandemic partly explains the observed increases.
Consumption decreased in almost all classes of antibiotics, except for the sulfonamide and trimethoprim family and the tetracycline family.
Consumption and prescriptions of nitrofurantoin have declined sharply and shifted toward fosfomycin.
Amoxicillin and the combination of amoxicillin with an enzyme inhibitor were the most prescribed and most consumed antibiotics throughout the entire period.
Antibiotic consumption in nursing homes with an in-house pharmacy
The data presented are from a national survey conducted by Mission SPARES on antibiotic consumption among residents in nursing homes (EHPADs) that have an in-house pharmacy (PUI).
What will antibiotic consumption be in 2022?
Total consumption in participating nursing homes is estimated at 30.7 Defined Daily Doses (DDD) per 1,000 resident-days (RD).
What changes occurred between 2018 and 2022?
Overall antibiotic consumption decreased by 10% compared to 2018 (34 DDD/1,000 ODN in 2022, 38.2 in 2018) in a cohort of 220 nursing homes with in-house pharmacies that submitted data annually.
In nursing homes, amoxicillin-clavulanic acid and amoxicillin are the most commonly used antibiotics, accounting for 35% and 24% of antibiotics, respectively, in 2022. It should be noted that the amoxicillin-clavulanic acid combination is, according to the SPILF classification, an antibiotic with “restricted indications, having a greater impact on bacterial resistance.” Due to the significant share of this antibiotic in total consumption, the proportion accounted for by these “restricted-use” antibiotics is the highest in nursing homes and even increased between 2018 and 2022 from 53% to 56%.
Conversely, azithromycin consumption remains higher in 2021 than in 2018 and 2019. The management of COVID-19 patients, in whom bacterial pneumonia was sometimes suspected, explains the increase in the use of ceftriaxone and azithromycin, particularly at the start of the pandemic. However, it is lower in 2021 than in 2020, in line with the recommendations issued for the management of COVID-19-positive patients.
Continued vigilance is needed regarding infections caused by antibiotic-resistant Enterobacteriaceae
In healthcare facilities
The incidence of infections caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae isolated from all diagnostic specimens collected in healthcare facilities increased from 27 to 71 cases per 100,000 hospital days between 2008 and 2016. Starting in 2016, a decline began, with 67 cases in 2017, 63 cases in 2018, and 53 cases in 2019 (using a slightly different method) per 100,000 hospital days. However, in 2020, the incidence of VRE increased again to 58 cases per 100,000 hospital days in the context of the COVID-19 pandemic. In 2022, the incidence returned to a level similar to that of 2019, with 54 cases per 100,000 hospital days.
In healthcare facilities, the proportion of fluoroquinolone resistance among E. coli strains isolated from invasive infections was 14.7% in 2022. Overall, this rate has been declining since 2012.
Efforts to control cross-transmission and improve antibiotic use in healthcare facilities must therefore be pursued relentlessly to reinforce this positive trend.
The incidence rates (IR) of MRSA observed in 2022 were lower than in 2021. The IR of VRE was higher than it was in 2022 (
Over the 2018–2022 period, the MRSA IR began a new decline. The trend for EBLSE is generally stable between 52 and 54 cases per 100,000 hospital days, with a one-time increase to 58 cases in 2020.
Trends in the incidence (number of strains per 1,000 hospital days) of MRSA and EBLSE between 2002 and 2022 (the number of participating facilities varies each year; the surveillance method changed in 2018)
 of MRSA and EBLSE between 2002 and 2022 (the number of participating facilities varies each year; the surveillance method changed in 2018)")
rapport/synthèse
21 November 2023
Preventing Antibiotic Resistance: A "One Health" Approach - November 2023
enquêtes/études
24 November 2023
Monitoring of Antibiotic Use and Bacterial Resistance in Healthcare Facilities. Spares Project. Summary Results, 2022
Progress has been made in both community settings and nursing homes regarding resistance to third-generation cephalosporins, but vigilance is needed regarding resistance to fluoroquinolones
Decrease in E. coli resistance to third-generation cephalosporins (3GC) in community settings and nursing homes
Escherichia coli is the most frequently isolated bacterium in community laboratories (9 out of 10 bacteria): it is particularly responsible for urinary tract infections.
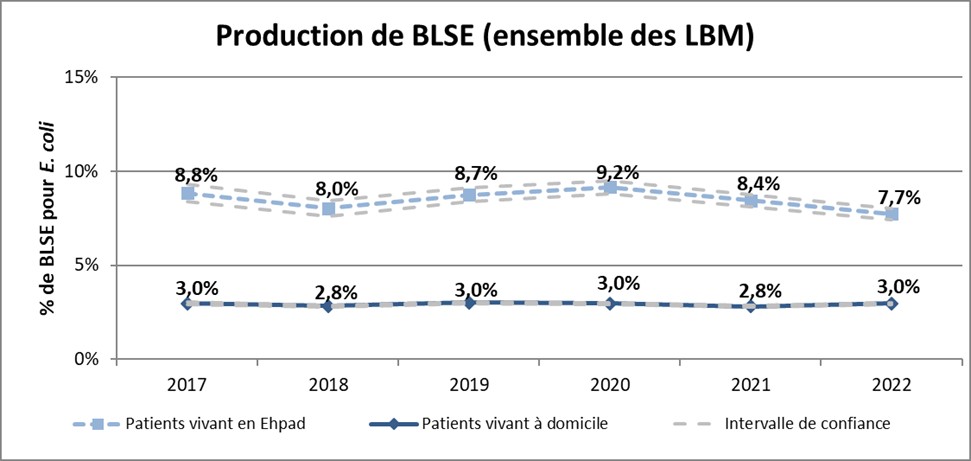
In community settings, the proportion of third-generation cephalosporin resistance among E. coli strains isolated from urine samples was 3.3% of all isolated strains in 2022. It increased from 2.3% in 2012 to 4.2% in 2015. It decreased from 4.2% in 2015 to 3.2% in 2018. Since then, it has remained stable between 3.2% and 3.4%. At the same time, the proportion of strains producing extended-spectrum beta-lactamases has remained relatively stable over the 2017–2022 period, ranging from 3.0% to 2.8% (3.0% in 2022).
In nursing homes, the proportion of third-generation cephalosporin resistance among E. coli strains isolated from urine samples is higher than among outpatients. It affected 8.5% of strains in 2022. After rising sharply from 8.0% in 2012 to 11.1% in 2015, this proportion was decreasing compared to 2017 (9.9%).
Trends between 2017 and 2022 in ESBL-producing E. coli strains isolated from urine samples in patients living at home and in nursing homes, France, Mission Primo
Increase in urban areas and decrease in nursing homes in fluoroquinolone resistance
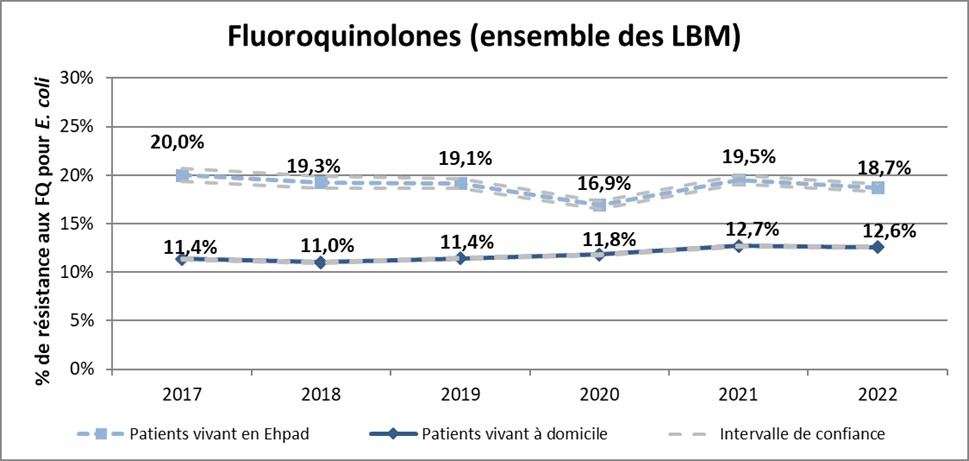
In the community, the proportion of fluoroquinolone resistance among E. coli strains isolated from urine samples was 12.6% of all isolated strains in 2022. It showed a downward trend from 12.5% in 2013 to 11.0% in 2018, but has been on the rise since 2018, with a more pronounced increase in 2021 (+7.6% compared to 2020).
In nursing homes, the proportion of fluoroquinolone resistance among E. coli strains isolated from urine samples accounted for 18.7% of strains in 2022. After a sharp decline from 27.8% in 2013 to 16.9% in 2020, the increase observed in 2021 appears to be a one-off rise that is not continuing into 2022.
These results show that the fight against antibiotic resistance remains a major public health challenge.
Trends between 2017 and 2022 in the proportion of fluoroquinolone resistance in E. coli isolated from urine samples in patients living at home and in nursing homes, France, Mission Primo
rapport/synthèse
13 November 2023
Antibiotic Use in the Private Sector in France, 2012–2022
rapport/synthèse
21 November 2023
Preventing Antibiotic Resistance: A "One Health" Approach - November 2023
enquêtes/études
24 November 2023
Monitoring of bacterial antibiotic resistance in community care and long-term care facilities. Primo National Initiative. Summary Results, 2022
The Situation in Europe
At the European level, data are available through the EARS-Net network for two species of Enterobacteriaceae: Escherichia coli (an Enterobacterium found in the digestive tract and frequently responsible for infections, primarily urinary tract infections) and Klebsiella pneumoniae.
In both of these bacterial species, the proportion of resistance to third-generation cephalosporins has risen sharply since 2006.
In 2021, the average proportion (weighted by the population of the countries participating in the network) of resistance to 3G cephalosporins in Escherichia coli was 14.3%. At 8.4%, France is below the European average. Over the 2018–2022 period, the average European proportion of resistance to third-generation cephalosporins in E. coli decreased from 15.7% to 14.3%. In France, the trend is also downward, as the proportion was 10.2% in 2017.
Regarding Klebsiella pneumoniae, the average proportion (weighted by the population of the countries participating in the network) of resistance to 3G cephalosporins is 32.7%. Over the 2018–2022 period, the average European proportion of resistance to third-generation cephalosporins in K. pneumoniae is declining (34.4% in 2018). In France, the trend is also downward, with 30.8% in 2018 and 25.0% in 2022.
Proportion of resistance to third-generation cephalosporins among Klebsiella pneumoniae strains isolated from invasive infections, Europe, 2022.
Proportion of third-generation cephalosporin resistance among Klebsiella pneumoniae strains isolated from invasive infections, Europe, 2022

A steady decline in methicillin-resistant Staphylococcus aureus (MRSA)
The situation is more favorable for methicillin-resistant Staphylococcus aureus (MRSA), as there has been a steady decline in MRSA infections between 2003 and 2022.
In 2022, the Spares study reported a MRSA incidence of 0.14 strains per 1,000 patient-days, with a rate nearly four times higher in the ICU, and the incidence of EBLSE was 0.54 strains per 1,000 patient-days, with a rate six times higher in the ICU.
Trends between 2002 and 2022 in the incidence (number of strains per 1,000 patient-days) of MRSA and EBLSE (number of participating facilities varies each year; change in surveillance method in 2018).
Trends in the incidence (number of strains per 1,000 hospital days) of MRSA and EBLSE between 2002 and 2022 (the number of participating facilities varies each year; the surveillance method changed in 2018)
 of MRSA and EBLSE between 2002 and 2022 (the number of participating facilities varies each year; the surveillance method changed in 2018)")
rapport/synthèse
21 November 2023
Preventing Antibiotic Resistance: A "One Health" Approach - November 2023
enquêtes/études
24 November 2023
Monitoring of Antibiotic Use and Bacterial Resistance in Healthcare Facilities. Spares Project. Summary Results, 2022
At the European level, the EARS-Net network reports an average rate (weighted by the population of the countries participating in the network) of methicillin resistance in Staphylococcus aureus of 15.2% in 2022. At 10.4%, France is slightly below the European average. Over the 2018–2022 period, the average European rate of methicillin resistance in Staphylococcus aureus decreased from 17.8% in 2018 to 15.2% in 2022.
It has also decreased in France.
Proportion of methicillin-resistant Staphylococcus aureus strains isolated from invasive infections, Europe, 2022

Risk of a therapeutic dead end: emerging highly antibiotic-resistant bacteria
Emerging highly resistant bacteria (EHRB) are bacteria naturally present in the human body that have become resistant to virtually all antibiotics commonly used to treat them. This makes it very difficult, if not impossible, to treat patients with EHRB infections.
Two types of bacteria are defined as HRAB: carbapenemase-producing Enterobacteriaceae (CPE), and glycopeptide-resistant Enterococcus faecium (GREF). In France, there are specific guidelines for the management of patients infected with or carrying HRAB, an updated version of which was published in January 2020.
Each year, Santé publique France conducts an assessment of the MRBA situation in France based on data from the external reporting system for healthcare-associated infections.
Since 2012, the number of reports of EPC or ERG has been steadily increasing. However, in the context of the COVID-19 pandemic, 2020 saw a significant decrease in reports of EPC (-38%) and ERG (-45%).
In 2022, reports (SIN) of healthcare-associated infections (HAIs) increased again, particularly those of healthcare-associated pneumonia (HAP), exceeding the number of SINs from 2019. The decrease in the number of SINs for episodes involving one or more HAIs observed in 2020 and 2021 can be explained by several hypotheses: 1) a decrease in the transmission of BHRe due to the enhanced control measures implemented for the COVID-19 pandemic; 2) a decrease in contact tracing around cases; or 3) probable underreporting of BHRe reports in favor of the very numerous COVID-19 reports.
Trends in the number of external reports of healthcare-associated infections involving carbapenemase-producing Enterobacteriaceae (CPE) submitted via the E-sin application in France. Data from 2012 to 2022
 submitted via the E-sin application in France. Data from 2012 to 2022")
Trends in the number of external reports of healthcare-associated infections involving glycopeptide-resistant Enterococcus faecium (ERG) submitted via the E-sin application in France. Data from 2012 to 2022
 submitted via the E-sin application in France. Data from 2012 to 2022")
References to a link to a foreign country were more frequent in 2022 than in 2021 and 2020.
The proportion of clinical specimens collected for diagnostic purposes is increasing, suggesting a decrease in the identification and/or investigation of colonized cases.
There has been a decrease in the implementation of enhanced contact precautions upon admission of cases, as well as in specific measures upon identification of a case, particularly for EPC.
Finally, monitoring of PROPIAS indicators shows that the proportion of secondary cases among EPC and ERG cases has increased.
These findings raise concerns about the risk of unidentified spread of EPC and ERG. Vigilance and efforts to control the spread of BHRe in healthcare facilities must be strengthened.
These data should be considered alongside those available from surveillance networks: French data from the EARS-net network show that the proportion of carbapenem resistance among Enterobacteriaceae isolated from blood cultures or CSF has remained below 1% for several years.
EPCs and ERGs are responsible for only a small number of serious infections in France. The latest survey on the prevalence of healthcare-associated infections in healthcare facilities (ENP) also reported that in 2017, 0.65% (95% CI [0.26–1.60]) of the Enterobacteriaceae tested were carbapenem-resistant, corresponding to a prevalence of patients infected with carbapenem-resistant strains of 0.01% (95% CI [<0.01–0.03]). Regarding ERG, the proportion of glycopeptide resistance among strains isolated from blood cultures is again less than 1%. Similarly, the ENP shows a glycopeptide resistance rate of 5.07% (95% CI [2.16–11.43]) among E. faecium strains. This corresponds to a prevalence of patients infected with glycopeptide-resistant E. faecium of less than 0.01%. An update of these prevalence rates based on the ENP conducted in May–June 2022 will be available shortly.
This situation is made possible by the promotion of the “search and isolate” strategy, implemented in French healthcare facilities following the recommendations of the High Council for Public Health (HCSP) updated in 2020 (originally published in 2013), to prevent the spread of MDR-E. faecium. However, the latest data from the National Reference Center (CNR) on antibiotic resistance urge us to remain vigilant. Efforts to control the spread of EPC and ERG in healthcare facilities remain relevant and must even be strengthened, especially since, more generally, the screening strategy appears to be shifting in 2020, in the context of the COVID-19 pandemic, raising concerns about a low-level spread of BHRe.
Resistance data for other common pathogens
The table below summarizes the latest available data for the main bacterial species pathogenic to humans that are the subject of specific thematic reports. Resistance phenomena in these species are of public health concern given the treatment failures they can cause.
The data presented here are primarily derived from surveillance networks coordinated by the CNRs in collaboration with Santé publique France.
Pathogen |
Main indicator of resistance |
% within the species |
Year |
Geographic coverage |
Sources |
File |
|---|---|---|---|---|---|---|
BACTERIA |
|
|||||
|
erythromycin ciprofloxacin |
8 68 |
2018 |
National |
- CNR Campylobacter and Helicobacter - Public Health France |
||
|
erythromycin ciprofloxacin |
0.5 55 |
2018 |
national |
- CNR Campylobacter and Helicobacter - Santé publique France |
||
|
glycopeptides ampicillin/amoxicillin (I+R) |
<1 0.3 |
2018 |
national |
- Onerba - Laboratory affiliated with the CNR for enterococci - CNR for antibiotic resistance - Santé publique France |
|
|
|
glycopeptides ampicillin/amoxicillin (I+R) |
<1 79.4 |
2018 |
national |
- Onerba - Laboratory affiliated with the CNR for enterococci - CNR for antibiotic resistance - Santé publique France |
|
|
|
3rd-generation cephalosporin fluoroquinolones carbapenems |
9.6 16.3 <0.1 |
2018 |
National |
- Onerba - BMR-Raisin - Public Health France |
|
|
amoxicillin |
22.0 |
2018 |
national |
- CNR Haemophilus influenzae - Public Health France |
|
|
|
third-generation cephalosporins carbapenems |
30.8 0.5 |
2018 |
national |
- Onerba - Public Health France |
|
|
multidrug resistance* |
1.9 |
2017 |
national |
- CNR Mycobacteria and Mycobacterial Resistance to Antituberculosis Drugs - Santé publique France |
|
|
|
ceftriaxone >0.125–0.25 mg/L >0.25 mg/L |
0 0 |
2018 |
National |
- National Reference Center for Gonococci - Public Health France |
|
|
|
penicillin G (I+R) rifampicin |
46 0.6 |
2018 |
National |
- Meningococcal National Reference Center - Santé publique France |
||
|
ceftazidime carbapenems |
13.0 16.0 |
2018 |
national |
- Onerba - Public Health France |
|
|
|
third-generation cephalosporin (children) and ciprofloxacin (adults) |
0 1 |
2018 |
national |
- CNR on Salmonella - Public Health France |
||
|
third-generation cephalosporin (children) and ciprofloxacin (adults) |
4.2 1.1 |
2016 |
national |
- CNR for Salmonella - Public Health France |
||
Salmonella enterica serotype 1,4,[5],12:i:- (monophasic variant of S. Typhimurium) |
third-generation cephalosporin (children) and ciprofloxacin (adults) |
0 0.9 |
2016 |
national |
- CNR for Salmonella - Public Health France |
|
|
ciprofloxacin azithromycin |
13.1 20.6 |
2017 |
national |
- CNR for Escherichia coli and Shigella - Public Health France |
|
|
Methicillin |
12.1 (in healthcare settings) |
2018 |
national |
- Onerba - BMR-Raisin - CNR for Staphylococci - Public Health France |
|
|
|
penicillin G (I+R) erythromycin (I+R) |
29.3 25.2 |
2018 |
national |
- National Reference Center for Pneumococci - Santé publique France |
||
|
erythromycin Adults Children Tetracycline |
3 2 4 11 |
2018 |
National |
- CNR for Streptococci - Onerba - Public Health France |
|
|
YEAST |
|
|||||
|
fluconazole voriconazole |
0 0 |
2017 |
regional |
- CNR Mycology and Antifungals |
|
|
|
fluconazole voriconazole |
see fact sheet |
2017 |
Regional (Ile-de-France) |
- CNR Mycology and |
||
Antibiotic-resistant bacterial strains are strains for which there is a high probability of treatment failure regardless of the type of treatment and the dose of antibiotic used. Resistance breakpoints for various antibiotics for each bacterial species are defined annually by the Antibiogram Committee of the French Society of Microbiology (CA-SFM). However, different resistance breakpoints may be adopted to ensure data comparability with international data (see Neisseria gonorrheae). For antifungals, the interpretation breakpoints used by the CNR are those defined by the CLSI (Clinical and Laboratory Standards Institute) pending those from the EUCAST committee.
The Burden of Antibiotic-Resistant Bacterial Infections in France and Europe
Raising awareness of the public health impact of antibiotic resistance is complex: surveillance systems target specific bacteria-antibiotic pairs and are sometimes even limited to certain types of specimens. It is difficult to help a non-professional audience understand what, for example, the incidence of diagnostic samples testing positive for MRSA (Methicillin-resistant Staphylococcus aureus)—one of the most common bacteria-antibiotic pairs encountered in hospital settings—actually means. It is therefore necessary to have complementary indicators that allow the subject to be addressed in a comprehensive manner and are more easily understood by everyone. This is the purpose of this European study, coordinated by the European Centre for Disease Prevention and Control (ECDC), in which Santé publique France participated, which aimed to estimate the number of cases, the number of deaths, and the number of DALYs (Disability-Adjusted Life Years) attributed to multidrug-resistant bacterial infections in Europe. The DALY indicator accounts for the total number of years lost due to death or disability, in this case as a result of a multidrug-resistant bacterial infection. It thus has the advantage of taking into account the duration of life impacted by a disease prior to death. The World Health Organization uses it in other studies on the global impact of diseases. This makes it possible to compare the burden of different diseases, which can help prioritize prevention efforts.
The Burden Study
Prior to the European study, a French study had already been conducted by Santé publique France to estimate the number of cases and deaths linked to multidrug-resistant bacterial infections that occurred in France in 2012.
The Burden BMR study conducted by Santé publique France in 2014–2015 aimed to estimate the public health burden (morbidity, mortality) of multidrug-resistant bacterial infections in France. Seven multidrug-resistant bacteria were selected for this study: methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, Escherichia coli and Klebsiella pneumoniae resistant to third-generation cephalosporins (3GC), K. pneumoniae, Acinetobacter spp., and carbapenem-resistant Pseudomonas aeruginosa. The incidence of invasive infections caused by these MDR bacteria (EARS-Net data, 2012) was adjusted and extrapolated to other sites of infection, and the mortality attributable to these infections was estimated using ratios from the literature.
Three key figures to remember:
158,000 cases of MDR infections per year in France, including 16,000 invasive infections (serious infections: meningitis, bacteremia, sepsis);
12,500 deaths associated with these infections;
The Burden BMR study confirms that the burden of MRB infections is very significant; MRSA and C3G-resistant Enterobacteriaceae infections account for the largest share (two-thirds of all recorded infections).
In relation to

Healthcare-associated infections
thematic dossier
Santé publique France is tasked with monitoring and preventing these infections in healthcare facilities, long-term care facilities, and community healthcare settings, thereby helping to limit...