
Post-Occupational Surveillance Program for Workers Exposed to Asbestos (ESPrI)
There is little health surveillance data in France on self-employed artisans, and even less on those who have retired. This is why the ESPrI program was launched.
In France, between 13,000 and 29,000 of the 280,000 new cancer cases diagnosed each year are believed to be work-related. Although these cancers most often develop after retirement, there is currently no standardized system for post-occupational monitoring of individuals enrolled in the various Social Security schemes. A regulatory framework for post-occupational monitoring of employees exposed to asbestos during their work has existed since 1995 but is still rarely implemented due to a lack of awareness.
Following recommendations from the InVS in 2001 (the "Espaces" study), the Social Security Scheme for the Self-Employed (RSI) asked the InVS in 2003 to establish the ESPrI program to monitor retired tradespeople who had been exposed to asbestos during their professional careers, based on the recommendations of the 1999 Consensus Conference on the medical monitoring of people exposed to asbestos (the only existing reference standard).
The effects of asbestos on the health of the French population are still being felt today. Between 13,000 and 29,000 new cancer cases each year are believed to be caused by occupational carcinogens. Santé publique France (formerly InVS) has developed monitoring and epidemiological surveillance systems specifically focused on occupational risks related to asbestos. Thus, particular attention must be paid to self-employed workers (artisans, merchants, and independent professionals) who do not have an occupational physician and cannot benefit from the post-occupational medical follow-up system intended for employees (Article D 461-25 of the Social Security Code).
The ESPrI program (Epidemiology and Surveillance of Self-Employed Workers) was created following the recommendations of the Espaces study published in 2001, and at the initiative of the Social Security System for the Self-Employed (which became the National Delegated Fund for Social Protection of the Self-Employed on January 1, 2018). The overall objective of this program was to develop and implement a surveillance system for the population of self-employed workers exposed to occupational carcinogens. Initially, the program focused on asbestos and craftsmen, with the following objectives:
Post-occupational monitoring (CNIL Opinion No. 05-113)
identify retired craftsmen who were exposed to asbestos during their professional careers, in order to inform them and provide them with medical follow-up;
to estimate, based on observed data, the prevalence of occupational asbestos exposure among the artisan population, and to describe it by gender, sector of activity, and occupation;
Epidemiological monitoring (CCTIRS Opinion No. 11-465, CNIL Opinion No. 911-447)
to explore the health effects of past exposures;
assess the impact of the program in terms of social benefits for artisans who have access to the Asbestos Victims Compensation Fund (FIVA).
ESPrI’s recruitment program was based on a network comprising the funds of the former RSI, covering 22 departments*.
Five invitation campaigns were launched between 2005 and 2009 in the Southwest, and two campaigns were conducted in regions further north in 2008 and 2009, targeting new retirees from the previous year. In 2010, the invitation campaigns were suspended and have not resumed since.
The Occupational Health Directorate (DST) of Santé publique France coordinates the program. The Occupational Pathology Consultation (CPP) at Pellegrin Hospital (Bordeaux) and the CPP at Côte de Nacre Hospital (Caen)—referred to as expert centers—were responsible for assessing occupational exposure to asbestos based on the full range of professional careers reported by retirees.
A self-administered postal questionnaire completed by the retiree was used to collect sociodemographic characteristics, work history, the frequency of performing work tasks potentially exposing them to asbestos, and their perception of any prior exposure. The assessment of the professional career was conducted by two occupational hygienists and was based on the criteria of the 1999 Consensus Conference, which classified each job into four exposure categories: high, moderate, low, and unexposed. Subsequently, each subject was classified according to the highest exposure category encountered during their career. A medical evaluation offered to subjects classified as “intermediate” or “high” exposure included an initial consultation with a physician of their choice, a chest CT scan, and a second consultation to complete the evaluation. Two medical questionnaires (“evaluation” and “CT scan”) were completed by the physicians.
* The departments covered by the ESPrI program are as follows: Dordogne (24), Gironde (33), Landes (40), Lot-et-Garonne (47), Pyrénées-Atlantiques (64), Corrèze (19), Creuse (23), Haute-Vienne (87), Charente (16), Charente-Maritime (17), Deux-Sèvres (79), Vienne (86), Calvados (14), Manche (50), Orne (61), Eure (27), Seine-Maritime (76), Nord (59), Pas-de-Calais (62), Aisne (02), Oise (60), Somme (80). They cover the regions of Nouvelle-Aquitaine, Normandy, and Hauts-de-France.
Epidemiological monitoring
Epidemiological monitoring is structured around three components: mortality, morbidity, and finally the medico-social component, which includes an analysis of Fiva utilization.
It is conducted passively, using data extracted from medical-administrative databases: vital status data comes from the National Registry of Natural Persons (RNIPP), causes of death data from the Center for Epidemiology on Medical Causes of Death (CepiDC), morbidity data from the National Inter-Regime Health Insurance Information System (Sniiram), and compensation data from the Fiva databases.
Each respondent to the self-administered questionnaire had the option to decline participation in one or more components of the epidemiological surveillance. Consequently, the size of the cohort varies for each of the three components.
The operational implementation of the passive epidemiological surveillance of the ESPrI cohort has been in effect since 2012.
Regular updates to data from the RNIPP and Cépidc make it possible to describe mortality among retired craftsmen and its causes relative to the general French population. It also allows for estimating the risks of cancer-related death among artisans based on sociodemographic and socio-professional characteristics, as well as exposure to asbestos or silica (gender, age, occupations, sectors, exposure indicators, etc.), for several cancer sites (lung, colon, ovary, larynx, pleura, etc.).
Monitoring of the occurrence of diseases linked to the carcinogens studied is conducted using annual data extracts from the Sniiram (CNAM) databases, in which cancer diagnoses are identified through the application of algorithms.
Fiva was established in 2002 to supplement the occupational disease recognition system and, in particular, to enable all asbestos victims and their beneficiaries to have their exposure recognized, as self-employed workers are not eligible for occupational disease recognition.
Operational data transfer diagram since 2012
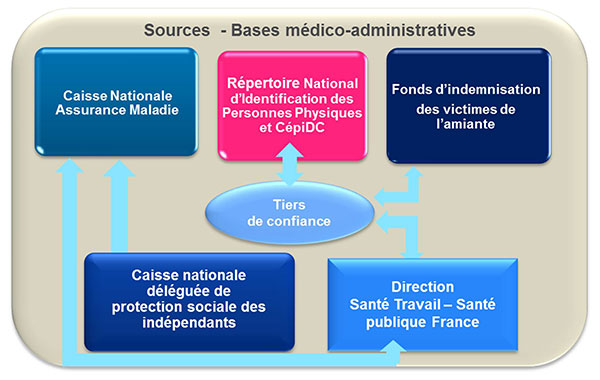
The Villejuif Center for Epidemiology and Public Health served as a trusted third party for the program until 2017 – The Social Security System for the Self-Employed became the National Social Security Fund for the Self-Employed on January 1, 2018.
For research purposes, Santé publique France wishes to make the data from this program available as part of an open-data policy. The research community and other parties may request access to a portion of the ESPrI program data.
This includes:
occupational data (complete career histories of indicators of exposure to asbestos and silica: intensity, frequency, probability, duration, cumulative index, exposure level, etc.);
morbidity data: data on healthcare utilization, medication use, etc., regarding the history of long-term conditions and hospitalization data;
mortality data: vital status, dates, and causes of death.
For more information: Data provided by Santé publique France. Epidemiological data on retired artisans from the ESPrI program.