
PANJO Initiative: Early Prevention, Evidence-Based Practices, and Maternal and Child Health Services
Everything You Need to Know About the PANJO Program, Which Is Offered to Expectant Parents Living in Adverse Psychosocial Conditions to Help Foster the Development of an Attachment Bond with Their Newborn
Contact
For any questions or additional information, please contact: evalpanjo@santepubliquefrance.fr
The PANJO Initiative: Early Prevention, Evidence-Based Practices, and Maternal and Child Health Services
The quality of the relationship that develops between a parent and their newborn is crucial to the child’s future development and health. However, the living conditions in which parents welcome their babies vary and do not offer the same opportunities to everyone. That is why Santé publique France developed and piloted the PANJO early prevention intervention. It is offered to expectant parents living in an adverse psychosocial environment to promote the development of secure attachments.
The Attachment Bond
A young child’s need for emotional security is a fundamental need, just like eating or sleeping. The quality of a baby’s attachment to a parent will impact the child’s short- and long-term psycho-emotional development. The attachment bond is formed through daily interactions between a caregiver and the baby, particularly when the child is distressed and turns to the adult to regain a sense of security. The formation of secure baby-parent attachment bonds fosters the child’s autonomy, flexibility, and self-confidence as well as trust in others, thereby contributing to their overall development.
PANJO’s strategy is based on supporting parents from pregnancy through the child’s first 12 months. Midwives and pediatric nurses from the PMI make between 6 (minimum) and 12 home visits to expectant and new parents. What sets PANJO home visits apart is that they systematically devote a significant amount of time to observing the baby and parent-baby interactions, which helps foster secure attachments. The professional’s role is to support parents in developing their sensitivity, closeness, commitment, and ability to foster reciprocity with their child. These interventions are conducted exclusively by PMI professionals who have received PANJO training, use PANJO intervention tools, and receive supervision.

The first phase of PANJO, implemented by INPES (the National Institute for Prevention and Health Education, which became Santé publique France in May 2016), aimed to develop the PANJO intervention and test its acceptability among professionals in maternal and child health services and among beneficiary families in three departments. This initial phase confirmed that the program was very well received by professionals and families and allowed for its optimization.

The second phase made it possible to assess the appropriateness of the strategies for implementing this innovative intervention and to measure its effectiveness. To this end, Santé publique France signed a research and development agreement with the Agency for New Social and Health Interventions (ANISS).
Method
The Panjo 2 efficacy study included 330 women pregnant with their first child who reported feeling lonely during pregnancy. The 159 women who received support using the PANJO method constituted the exposed cohort. The control cohort consisted of 171 women receiving standard care available in France during the perinatal period. Participants were interviewed once at the end of their pregnancy at the time of recruitment, once when the child was six months old, and a final time at twelve months.
The data collected were intended to measure the effectiveness of PANJO home visits in promoting a sense of parental efficacy (primary outcome), reducing coercive parenting behaviors, promoting health-protective behaviors, and improving the appropriate use of medical and social services. These short-term effectiveness criteria are, in fact, predictors of the intervention’s long-term effectiveness on the child’s physical, cognitive, and psycho-emotional development.
Partners
Santé publique France and ANISS were able to count on the commitment of some twenty PMI teams spread across eleven departments to pilot the intervention with families in the exposed cohort. Eight maternity wards facilitated the recruitment of families for the control cohort. Other partners joined the project. We were thus able to rely on the Université du Québec à Montréal for scientific support, child and adolescent psychiatry services to provide supervision for the interventionists, the Federation of Perinatal Networks, and certain Regional Health Agencies (ARS) to support the local implementation of the study.
Results
Quantitative and qualitative implementation evaluations highlight the relevance of the support system for professional practices and identify certain challenges that must be addressed to ensure the intervention’s sustainability beyond the pilot phase.
The results of the effectiveness evaluation show that, at six months of age, the Panjo intervention has favorable effects on parent-infant interactions for certain groups of more vulnerable women: fewer hostile reactions toward the infant and fewer dysfunctional interactions. Positive effects were also observed regarding access to health care and preventive services: fewer emergency room visits for infants, fewer instances of mothers foregoing care, and greater satisfaction with the support received from maternal and child health centers (PMI). However, no effect was observed on the perception of parenting competence, the study’s primary outcome measure.
An initial presentation of the results was given at the French Public Health Society Congress in October 2021.

Support the changes in preventive practices necessary to implement PANJO
2022–2025: Pilot Implementation
The lessons learned from the PANJO 2 evaluation helped improve the intervention’s design, update the tools, and refine the training methods for future implementers.
The goal of the pilot rollout was to identify the best ways to work in partnership—between departments, Regional Health Agencies (ARS), and Santé publique France—to enable the large-scale and sustainable rollout of an optimized PANJO intervention. The lessons learned from this pilot will help define the guidelines for a rollout strategy for the rest of France.
More than 15 PMI services are participating in the pilot. As a result, 1,015 PMI home-visit providers have been trained in PANJO 3. The rollout can be organized at the departmental or regional level, as is the case with the initiatives of the ARS in Brittany and the ARS in Nouvelle-Aquitaine.
Training and supervision for midwives and pediatric nurses were co-funded by the ARS’s FIR, the “First 1,000 Days of a Child’s Life” policy, and agreements signed under the National Strategy for Child Prevention and Protection.
The results of the pilot program evaluation will be published in the first quarter of 2027.
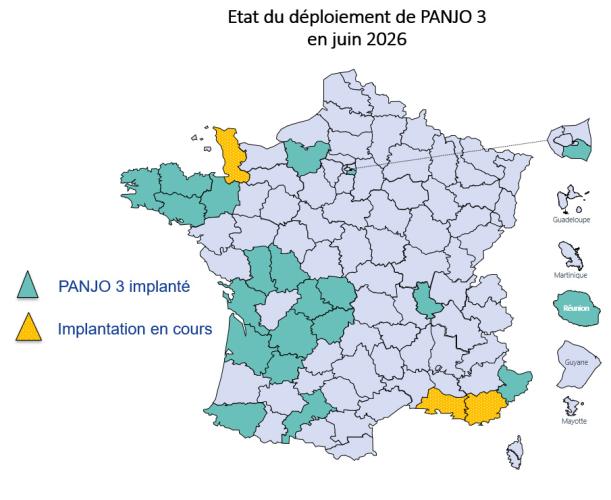
PMI services in 23 departments have implemented the PANJO 3 program in 8 regions. The program’s objectives remain unchanged. The goal is to promote the health and attachment of young children by offering (expectant) parents living in high-risk psychosocial environments 6 to 12 visits that will help them strengthen their ability to meet their baby’s emotional security needs.
In PANJO 3, Regional Health Agencies (ARS) and PMI supervisors receive methodological and scientific support provided by Santé publique France or one of its partners, such as the Institut de la parentalité.
Home-visit workers receive a 5-day training program to gain a better understanding of attachment theory and the PANJO intervention protocol, as well as to familiarize themselves with the tools. They participate in about ten group supervision sessions per year to provide long-term support in integrating professional practices based on attachment and collaboration with families.
Supervisors and practitioners participate in monitoring the program’s rollout and in evaluation studies conducted by Santé publique France.
References
Sylvia Garnier, Bénédicte Popineau, Panjo: Early Support for Parent-Infant Relationships, Volume 9467, Issue 391, 01/2025, Pages 1–46, ISSN 0007-9820,
Guillou A, Collet C, Corre R, Masson S, Sempe S, Bescond N. Newborn Behavioral Observation at Different Stages of the Perinatal Journey. Soins Pediatr Pueric. 2025;46(344):34-38.
- Taymi S., Popineau B., Estebanez L-A., Quéruel N., “Panjo Home Visits: Support Tailored to the Family and the Newborn.” Health in Action. Supporting the Formation of Early Parent-Child Bonds. May 2024, No. 466, pp. 24–26
- Sempé S., et al., “Early Prevention: Results of the Efficacy Study on the PANJO Intervention Tested by Eleven Maternal and Child Health Centers.” Santé Publique, 2022/HS1 (Vol. 34),
- Saïas T. “The PANJO Project: Managing the First 1,000 Days of Life Based on Professional Practices.” *Cahiers de la puéricultrice*—Vol. 59—No. 356—April 2022
- Mercerat C. et al., “The Panjo Program in France: A Qualitative Evaluation of Implementation and Changes in Professional Practices.” Revue Francophone Internationale de Recherche Infirmière – 2021 – No. 7
- Sempé S., “Panjo: Home Visits to Strengthen the Mother-Child Bond.” *La Santé en action*, *Children’s Basic Needs*, March 2019, No. 447, pp. 44–45.
- Saïas T. et al. “Supporting the Competencies of Early Intervention Practitioners in France: Uses and Effects of the Panjo Program.” Revue Francophone Internationale de Recherche Infirmière – 2019 – No. 5
- Lagarde C. “The Experience of Containment in Supervision Work with PMI Childcare Workers within the PANJO Program.” *Enfances et Psy* – 2018 – No. 77
- Le Nestour, A. “The PANJO Program: Intensifying Network Collaboration.” *Enfances et Psy* – 2016 – No. 69