
Summary of Legionnaires' disease cases reported in France in 2017
Number of reported cases and incidence
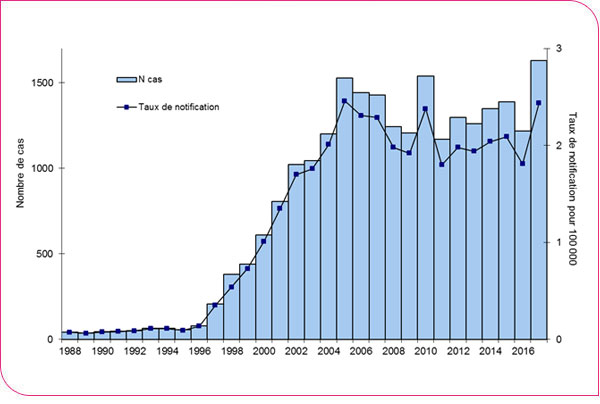
In 2017, 1,630 cases of Legionnaires’ disease were reported in France through the mandatory reporting system. Of these, 9 cases involved residents of the French overseas departments (1 case in Guadeloupe, 2 in Martinique, and 6 in Réunion), and 32 involved foreign nationals diagnosed in France. The incidence rate of reported cases of Legionnaires' disease in mainland France was 2.4 per 100,000 inhabitants. The number of cases reported in 2017 was significantly higher than in 2016, when 1,218 cases were reported (incidence of 1.8 per 100,000 inhabitants), and also slightly higher than in 2005 (1,527 cases) and 2010 (1,540) (Figure 1).
Figure 1. Trends in the annual number and incidence rate of reported cases of Legionnaires’ disease in France, 1988–2017
The west-to-east geographic gradient in the incidence rate of reported cases of legionellosis was pronounced, as observed in previous years, with incidence ranging from 0.8 per 100,000 inhabitants in Brittany to 4.2 per 100,000 inhabitants in Bourgogne-Franche-Comté (Figure 2). Based on the former regional divisions, the observed west-east gradient was more pronounced (Figure 3).
Figure 2. Distribution of the age- and sex-standardized* incidence rate of Legionnaires' disease by region of residence in mainland France, 2017
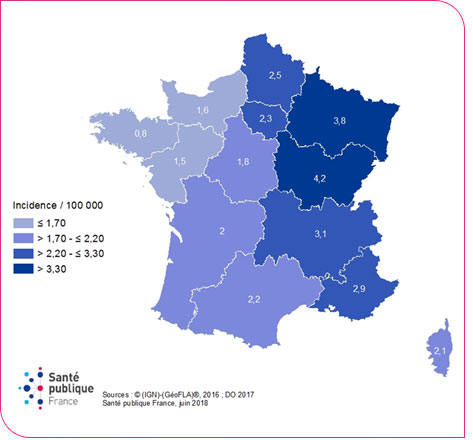
* Standardized by sex and age
Figure 3. Distribution of the age- and sex-standardized* incidence rate of Legionnaires’ disease by region of residence (former regional divisions) in mainland France, 2017
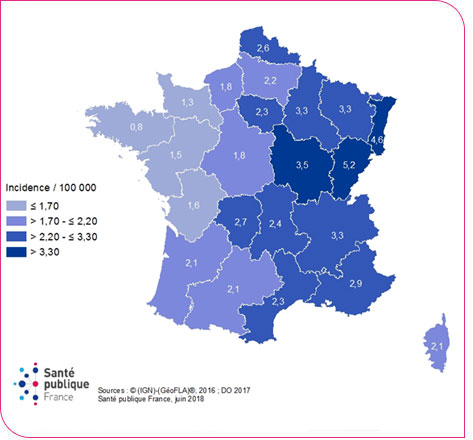
* Standardized by sex and age
Case characteristics
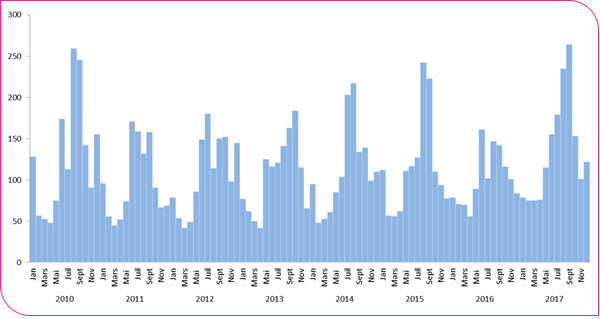
The median age of cases was 64 years [min-max: 19–99 years] and the male-to-female ratio was 2.4 (1,152 men and 478 women). Incidence increased with age, and the highest incidence rates were observed among people over 80 years of age (8.4 per 100,000) (Figure 4). Only 25 cases (out of 1,630 cases, 1.5%) were not hospitalized. The monthly number of cases remained high throughout the year but increased significantly starting in May, peaking in September with 265 reported cases (Figure 5).
Figure 4. Incidence rate by age group and sex of Legionnaires’ disease cases reported in France in 2017
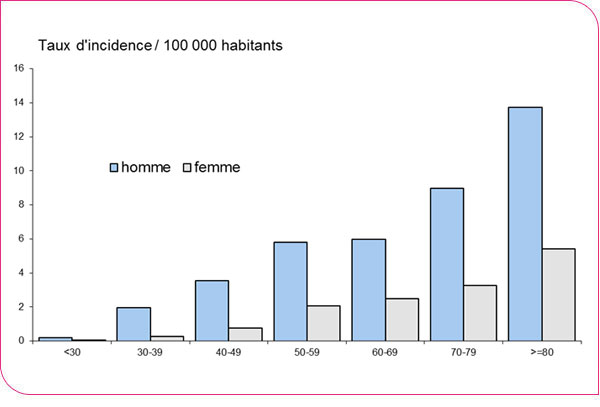
Figure 5. Number of reported cases of Legionnaires’ disease by month of symptom onset, France, 2010–2017
73% of cases (1,191/1,629) had at least one known risk factor (Table 1). For 31% of cases, smoking was the sole risk factor (8% had an additional factor).
Table 1. Frequency of risk factors for Legionnaires’ disease cases in France, 2015–2017 | ||||||
2015 (1,389) |
2016 (1,218) |
2017 (1,629) |
||||
Contributing factors* |
N |
% |
N |
% |
N |
% |
Cancer / blood disorder |
177 |
13 |
156 |
13 |
171 |
10 |
Corticosteroid therapy/immunosuppressants |
163 |
12 |
136 |
11 |
168 |
10 |
Diabetes |
261 |
19 |
223 |
18 |
303 |
19 |
Smoking |
615 |
44 |
533 |
44 |
640 |
39 |
Other |
239 |
17 |
213 |
17 |
300 |
18 |
At least one factor |
1,059 |
76 |
938 |
77 |
1191 |
73 |
*not mutually exclusive.
The disease course was known for 91% of cases (1,485/1,630), and the case fatality rate (132 deaths) was significantly lower than in 2016 (8.9% versus 11.9%, p < 0.01).The median time between the onset of initial clinical signs and notification to the Regional Health Agency (ARS) was 6 days (interquartile range [4–9]); 84% of cases were reported within 10 days of the onset of initial clinical signs, and 95% within 20 days. These annual indicators have remained stable since 2010.
Microbiological Information
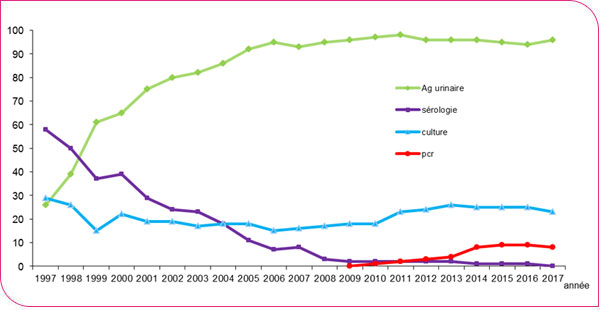
Of the 1,630 cases, 1,599 (98%) were confirmed cases, and detection of soluble urinary antigens was the primary diagnostic method used (1,571 cases, 96.4%). Genomic amplification (via Polymerase Chain Reaction—PCR) was performed for 128 cases (8%), and for 30 of these, PCR was the sole biological diagnostic method (32 in 2016). The proportion of cases diagnosed by PCR has not increased in recent years (Figure 6). The majority of cases were associated with Legionella pneumophila serogroup 1 (Lp1) (1,588/1,630).
Figure 6. Distribution of diagnostic methods for Legionnaires’ disease cases, France, 1988–2017
For 23.1% of cases (n=377), a strain was isolated; this percentage was comparable to that of 2016 (24.6%). The majority (373/377, 99%) of the isolated strains were L. pneumophila, including 361 Lp1 and 12 belonging to other serogroups. All these strains were analyzed using various molecular methods depending on the context (PFGE, sequence-based typing, or whole-genome sequencing (WGS)) at the National Legionella Reference Center. Among the Lp1 strains, 105 (29%) were so-called "endemic"* strains: 40 "Louisa" strains, 27 "Paris" strains, 22 "Lorraine" strains, 15 "Biarritz" strains, and 1 "Mondial" strain. Among the other Lp1 strains, 193 (54%) had a profile already listed in the CNR database, and 63 (17%) had a "sporadic" profile (not yet listed). Among the 383 cases for which a sequence type (ST) was available, 49% were associated with 8 STs: ST23, ST1, ST47, ST62, ST259, ST146, ST40, and ST20; the most common were ST23 (68 cases, or 18%) and ST1 (38 cases, or 10%). It should be noted that in the absence of strain isolation, complete "ST" genomic typing was performed directly on specimens for 10 cases (3 cases in 2016).For 64 cases (17%), the human strain could be compared to environmental strains isolated from one or more locations frequented by the patient, and for 49 of the 65 (75%) comparisons (1 case with 2 comparisons), the genomic profiles of the strains were found to be identical. Among these cases, environmental and microbiological investigations determined that the drinking water systems were the most likely source of contamination in 17 homes, 9 healthcare facilities, 9 tourism establishments, 5 nursing homes, and 4 other facilities. The results of the 5 other comparisons documented the involvement of a physical therapy practice as the source of contamination responsible for clusters of cases in Occitanie.
* Endemic strains: these strains comprise isolates with identical pulsotypes but isolated from cases with no epidemiological link
Risk exposures
A risk exposure during the incubation period (2–10 days) was reported for 633 cases (39%) (Table 2), a proportion comparable to that of 2016 (38%). The proportion of cases that had stayed in a hospital during the incubation period in 2017 (7%) was identical to that of 2016. Among these cases, 42% (50/118) were confirmed nosocomial cases (hospitalized throughout the presumed exposure period). The 13 cases who had visited a spa were isolated cases. The most frequently reported mode of exposure was still travel (299 cases, or 18%). Of these cases, 215 were reported to the European Legionnaires’ disease surveillance network (ELDSNet), of which 183 cases (11% of all cases) had stayed in a hotel or campground; the other reported cases had stayed in vacation rentals, guesthouses, or accommodations booked online. Of the 299 cases in which travel was reported, slightly more than one-third (108/299, or 35%) had traveled abroad, and most of these were to Europe (65/108 = 60%). In the "other exposures" category, 8 patients were using a continuous positive airway pressure (CPAP) device for sleep apnea (9 cases in 2016).
|
Table 2. Risk exposures among cases of Legionnaires' disease in France, 2015–2017 |
||||||
|---|---|---|---|---|---|---|
|
Exposures* |
2015 (1,389) |
2016 (1,218) |
2017 (1,630) |
|||
|
|
n |
% |
n |
% |
n |
% |
|
Hospital |
108 |
8 |
84 |
7 |
118 |
7 |
|
Retirement home |
55 |
4 |
54 |
4 |
87 |
5 |
|
Spa |
6 |
14 |
1 |
13 |
1 |
|
|
Travel |
304 |
22 |
219 |
18 |
299 |
18 |
|
Campground hotel |
177 |
13 |
141 |
12 |
189 |
11 |
|
Temporary residence |
84 |
6 |
36 |
3 |
83 |
5 |
|
Other types of travel* |
43 |
3 |
42 |
3 |
27 |
2 |
|
Others |
108 |
8 |
89 |
7 |
116 |
8 |
|
Total cases with at least one exposure |
581 |
42 |
460 |
38 |
633 |
39 |
a Rental property, bed-and-breakfast, vacation rental, second home, staying with friends or family
b No details provided regarding location or type of accommodation
c Public facilities (swimming pool, stadium, etc.), occupational exposure, sleep apnea device, etc.
In 2017, the European ELDSNet network reported 60 additional cases to Santé publique France beyond those reported through mandatory reporting (compared to 29 in 2016 and 59 in 2015). These were cases occurring among foreign nationals who had stayed at a tourist facility in France within 10 days prior to the onset of symptoms and were diagnosed in a foreign country. In total, based on notifications of French and foreign cases, 234 French establishments were reported by ELDSNet (156 in 2016 and 264 in 2015), 215 for isolated cases and 19 for cluster cases (defined by ELDSNet as at least two cases having stayed in the same establishment over a two-year period). In these 19 facilities, an investigation involving water sampling from the potable water system revealed the presence of Legionella above the regulatory threshold in 9 (47%) of them. In 2016, several investigations of clustered cases—both temporally and spatially—were conducted by the ARS in collaboration with the Cires. Most investigations failed to identify common sources of contamination. Three investigations were reported to national authorities. One investigation concerned recurring cases, dating back to 2013, linked to a stay at a hospital in Alsace. In the Pays de la Loire region, an investigation conducted following the occurrence of 4 cases in a nursing home identified the potable water system as the source of this outbreak. In Occitanie, 18 community cases had resided in the same urban neighborhood between January and July 2017. Eight of these 18 cases had visited a physical therapy clinic offering balneotherapy sessions. Epidemiological, environmental, and microbiological findings showed that the balneotherapy facility was the common source of infection for the cases, which could explain the majority of infections among people both inside and outside the clinic. Additionally, an outbreak of Pontiac fever was investigated in the Hauts-de-France region.
Conclusion
In 2017, the number of Legionnaires’ disease cases was significantly higher than in 2016 and slightly higher than in 2005 and 2010. The incidence rates of reported cases in mainland France in 2005, 2010, and 2017 are similar (between 2.4 and 2.5 per 100,000 inhabitants). These high rates are not due to an increase in cluster cases but to an increase in sporadic cases, as observed in the fall and winter of 2005 and in August and September 2010. The European notification rate for 2017 will be available on the ECDC website [2] during 2018. The number of cases reported by several countries in 2017 was also higher than in previous years, particularly in France’s neighboring countries (Italy and Spain), with a higher reporting rate than in France (Italy: 3.3 and Spain: 3.4 per 100,000 in 2017). The causes of this increase have not been identified. Indeed, compared to previous years, the characteristics of the cases and the diagnostic methods are identical, and no change in the virulence of Legionella strains has been reported. The "west-east" geographical gradient in the incidence rate of reported cases observed in recent years remains present. A multifactorial study analyzing meteorological factors showed that humidity and temperature are linked to the occurrence of Legionnaires' disease cases [3].
[1] Summary of Legionnaires' disease cases in France in 2016.
[2] European Centre for Disease Prevention and Control. Surveillance atlas of infectious diseases–Legionnaires' disease. [Internet]. Stockholm: ECDC, 2018.
[3] Camille Pelat, Christine Campese, Daniel Lévy-Bruhl, Didier CheSpatiotemporal disparities of Legionnaires' disease incidence in France: what part does climate play? EPIDEMICS 6 – the 6th International Conference on Infectious Disease Dynamics 29 November – 1 December 2017 Barcelona