Epidemiological Data 2008–2012
Key Points
Between 2008 and 2012, 4,584 patients with chronic hepatitis B who had not previously received antiviral treatment and were newly enrolled in 33 specialized hepatology units agreed to participate in the surveillance program.
Most were young adults (median age: 36 years), and predominantly men (59%); women were younger (34 years) than men (37 years)
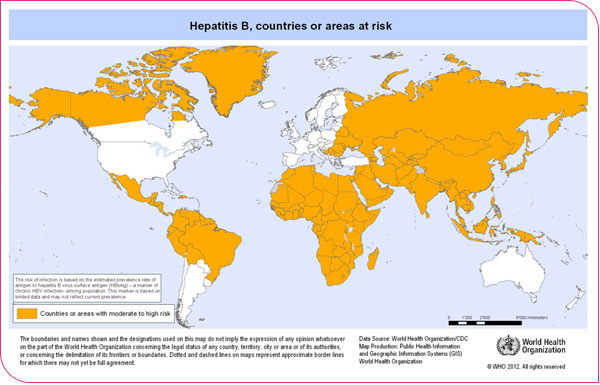
While 82% of patients were born in a country with moderate or high HBV endemicity, only a minority (13%) of them reported risk factor screening as the circumstance leading to the discovery of HBsAg positivity
more than two-thirds of patients are treated in a specialized unit in the year of or within one year following their first positive HBsAg test. Patients born in a country with low HBV endemicity (primarily those born in metropolitan France) are treated the latest after the discovery of seropositivity (more than three years later, for 40% of them)
Nearly 90% of patients are HBeAg-negative at the start of care; this proportion does not vary according to the HBV endemicity of the country of birth
While 59% of patients have a low HBV viral load (< 2,000 IU/mL), this viral load is very high (> 20,000 IU/mL) for the majority (79%) of HBeAg-positive patients and for 15% of HBeAg-negative patients
The main HBV genotypes are genotypes D (33%), E (28%), and A (24.5%)
Two-thirds of patients undergo an assessment of liver fibrosis at the start of care, performed using a non-invasive test in more than 70% of cases
Severe liver disease (cirrhosis or hepatocellular carcinoma) is diagnosed at baseline in 11% of patients
While antiviral treatment is initiated at the time of diagnosis in fewer than one-quarter of patients, the majority of patients presenting with severe liver disease at the time of diagnosis or a very high HBV viral load (≥ 20,000 IU/mL) are placed on treatment.
The majority of patients newly diagnosed with chronic hepatitis B in specialized hepatology departments are rarely screened for risk factors; the diagnosis is more often made during routine health checkups (general checkup, pregnancy). This contributes to delays in diagnosis and the implementation of preventive measures (particularly among at-risk individuals born in countries with low HBV endemicity) and could represent a missed opportunity for patients with chronic hepatitis B in France.
This is why it is essential to increase public information and raise awareness among physicians regarding the screening, prevention, and follow-up of chronic hepatitis B.
Participation of expert services
Thirty-three of 37 expert hepatology services participated in the surveillance of chronic hepatitis B between 2008 and 2012, and 26 participated continuously throughout the entire five-year period.
Patient participation
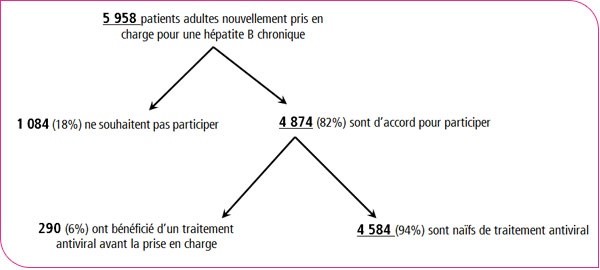
Between 2008 and 2012, 4,584 patients newly diagnosed with chronic hepatitis B in hepatology specialist units and who had not previously received antiviral treatment agreed to participate in the surveillance.
Patient gender and age at enrollment
Table 1 - Sex and age of patients at the start of care. Patients who had not previously received antiviral treatment and were newly diagnosed with chronic hepatitis B (N=4,584, specialized hepatology units, France, 2008–2012) | |||
Women |
Men |
Total |
|
n (%) |
1,866 (40.7) |
2,718 (59.3) |
4,584 |
Average age |
37 years |
39 |
38 |
DS1 |
± 13 years |
± 13 years |
± 13 years |
Median age |
34 years |
37 years |
36 years |
IQR2 (25%–75%) |
(27–43 years) |
(29–47 years) |
(28–46 years) |
(1) SD: standard deviation.
(2) IQR: interquartile range.
Mostly men (59%)
Median age: 36 years
Women are younger than men (p < 0.03)
Between 2008 and 2012, no significant changes were observed in epidemiological characteristics, in terms of age and sex of patients treated in hepatology specialty units that continuously participated in the surveillance (N=26 sites)
Patients’ continent of birth
Table 2: Distribution of patients by continent of birth. Antiviral-naive patients newly treated for chronic hepatitis B (specialized hepatology units, France, 2008–2012) | ||
Continent of birth |
Total N=4,340 |
|
|
n |
% |
Metropolitan France |
776 |
17.9 |
Overseas territories |
208 |
4.8 |
Europe excluding France: - Northern Europe - Western Europe - Eastern Europe - Southern Europe |
1 6 186156 |
0.0 0.1 4.3 3.6 |
North America |
2 |
0.0 |
South America + English- and Spanish-speaking Caribbean |
63 |
1.5 |
Pacific |
2 |
0.0 |
Sub-Saharan Africa |
1,869 |
43.1 |
North Africa |
335 |
7.7 |
Middle East |
187 |
4.3 |
Asia |
538 |
12.4 |
Indian Subcontinent |
11 |
0.3 |
The continent of birth is recorded for 4,340 (95%) patients. Among these patients,
18% were born in mainland France
nearly 8% in a North African country
43% in a sub-Saharan African country
12% in an Asian country
Distribution of patients according to HBV endemicity in the country of birth
Table 3: Distribution of patients by HBV* endemicity level in the country of birth. Antiviral-naive patients newly diagnosed with chronic hepatitis B (N=4,340, specialized hepatology units, France, 2008–2012) | ||
HBV endemicity zone |
Continent of birth |
Total n (%) |
Low endemicity (HBsAg prevalence < 2%) |
Metropolitan France, Northern Europe, Western Europe, North America |
785 (18) |
Moderate endemicity (HBsAg prevalence 2%–8%) |
Overseas departments and territories, Eastern Europe, Southern Europe, North Africa, the Middle East, the Indian subcontinent, South America, the English- and Spanish-speaking Caribbean, and the Pacific |
1,148 (26.5) |
High HBV endemicity (HBsAg prevalence ≥8%) |
Sub-Saharan Africa, Asia |
2,407 (55.5) |
*WHO classification
In total, over the 2008–2012 period,
82% of treatment-naive patients treated for chronic hepatitis B were born in areas of moderate or high HBV endemicity.
Between 2008 and 2012, in the 26 hepatology specialist departments that participated continuously in the surveillance
a gradual decrease in the proportion of patients born in areas of low HBV endemicity*: from 26% in 2008 to 13% in 2012 (p < 10⁻³)
an increase in the proportion of patients born in sub-Saharan Africa: from 39% in 2008 to 49% in 2012 (p < 10⁻³)
Age group and sex by HBV endemicity of country of birth
Figure 1 - Distribution of men by age group according to the HBV* endemicity level of the country of birth, among treatment-naïve patients newly enrolled for chronic hepatitis B (N=4,340, specialized hepatology units, France, 2008–2012)
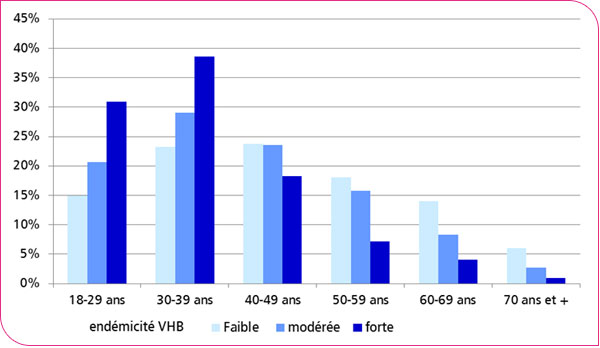
Figure 2 - Distribution of women by age group according to HBV* endemicity level in the country of birth, among antiviral-naïve patients newly enrolled for chronic hepatitis B (N=4,340, expert hepatology units, France, 2008–2012)
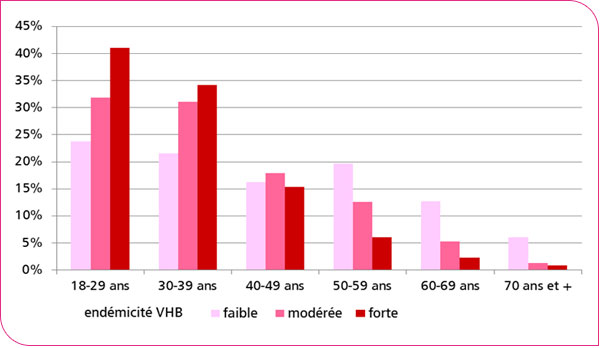
The median age of patients at the start of treatment varies according to the HBV endemicity level of the country of birth:
low HBV endemicity: 44 years
moderate HBV endemicity: 38 years
high HBV endemicity: 33 years
Men and women born in areas of low HBV endemicity are older at the time of diagnosis than men and women born in areas of moderate or high HBV endemicity.
*WHO classification
Circumstances of HBsAg detection according to HBV endemicity in the country of birth
A single circumstance of HBsAg positivity detection was reported by 3,216 patients: 70% of them discovered it during a routine screening (e.g., health checkup, pregnancy, blood donation) and 14% during diagnostic testing for clinical or laboratory findings. Only 13% reported having been screened for HBsAg based on risk factors.
Figure 3: Circumstances§ of HBsAg (+) detection, according to HBV* endemicity in the country of birth. Patients who had not previously received antiviral treatment, newly diagnosed with chronic hepatitis B (n=3,216, specialized hepatology units, France, 2008–2012).
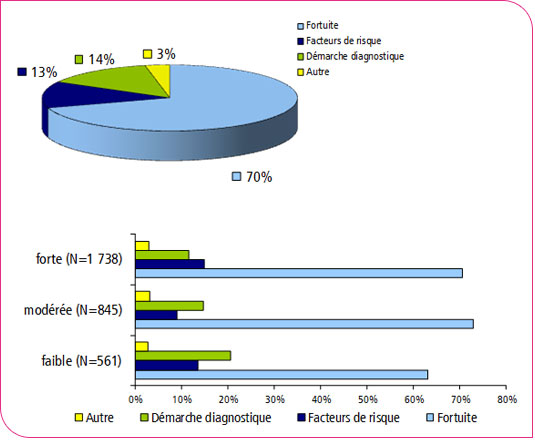
Screening for HBsAg due to risk factors is rarely (13%) mentioned by patients, including those born in a country with moderate or high HBV* endemicity.Risk factors: multiple sexual partners, close contact with a chronic HBsAg carrier, drug use, birth, prolonged stay, or medical care in a country with HBV endemicity…
1 Data limited to patients who reported only one circumstance of HBsAg(+) detection
*WHO classification
Time from detection of HBsAg positivity to initiation of treatment, according to HBV endemicity in the country of birth
Figure 4 - Time§ between detection of HBsAg (+) and initiation of treatment, according to HBV* endemicity in the country of birth. Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (n=3,716, specialized hepatology units, France, 2008–2012)
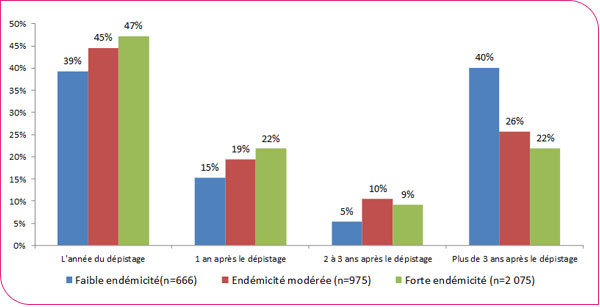
In total, 1,674 patients (45%) were treated within one year of the detection of HBsAg positivity.Patients born in areas of moderate or high HBV* endemicity are more often treated in the same year or the year following a positive screening result (64% and 69%, respectively) than patients born in areas of low endemicity (55%).
Compared to the average time to treatment for patients born in countries with high (2.7 years) or moderate (3.5 years) HBV endemicity, the average time to treatment for patients born in areas of low endemicity is significantly longer (6.7 years).
1 Time reported for 85%, 85%, and 86% of patients born in countries with low, moderate, and high HBV endemicity, respectively
* WHO classification
Comorbidities
Body Mass Index
Table 4: Body Mass Index (BMI) of patients, treatment-naïve, newly diagnosed with chronic hepatitis B (n=2,993, specialized hepatology units, France 2008–2012) | ||||||
|
Total (N=2,993) |
Men (N=1,822) |
Women (N=1,171) |
|||
|
n |
% |
n |
% |
n |
% |
BMI* < 25 kg/m² |
1,656 |
55.3 |
997 |
54.7 |
659 |
56.3 |
25 kg/m² ≤ BMI ≥ 30 kg/m²(overweight) |
898 |
30.0 |
599 |
32.9 |
299 |
25.5 |
BMI > 30 kg/m²(obesity) |
439 |
14.7 |
226 |
12.4 |
213 |
18.2 |
*BMI = weight/height²
Body Mass Index (BMI) was reported for 2,993 patients (65%).
One-third of patients are overweight
15% are obese (BMI > 30 kg/m²)
Women are more frequently obese at the start of treatment than men (18% vs. 12%, p < 0.03)
Excessive alcohol consumption
Table 5: Current or past excessive alcohol consumption*. Patients new to antiviral therapy, newly diagnosed with chronic hepatitis B (n=3,882, specialized hepatology units, France 2008–2012) | ||||||
|
Total (N=3,882) |
Men (N=2,283) |
Women (N=1,589) |
|||
|
n |
% |
n |
% |
n |
% |
Yes |
308 |
7.9 |
270 |
11.8 |
38 |
2.4 |
No |
3,574 |
92.1 |
2,013 |
88.2 |
1,551 |
97.6 |
*> 210g (21 drinks)/week for women, > 280g (28 drinks)/week for men
Excessive alcohol consumption was reported for 3,882 patients (85%).
8% of patients are heavy drinkers
Men are more likely to be heavy drinkers than women (12% vs. 2%, p<0.03)
Viral co-infections according to HBV endemicity in the country of birth
Table 6: HIV antibody positivity, by HBV* endemicity in the country of birth. Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (specialized hepatology units, France, 2008–2012) | ||||||||
HIV serology |
Total1 (N=3,350) |
Low prevalence (N=543) |
Moderate prevalence (N=862) |
High endemicity (N=1,855) |
||||
|
n |
% |
n |
% |
n |
% |
n |
% |
HIV-positive |
47 |
1.4 |
13 |
2.4 |
5 |
0.6 |
28 |
1.5 |
1 Documented HIV serology for 73% of patients (low endemicity 69%, moderate 75%, high 77%)
Table 7: HCV serological status, according to HBV* endemicity in the country of birth. Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (specialized hepatology units and hepatitis networks, France, 2008–2012) | ||||||||
Hepatitis C Serology |
Total1 (N=3,626) |
Low endemicity (N=608) |
Moderate endemicity (N=917) |
High endemicity (N=1,991) |
||||
|
n |
% |
n |
% |
n |
% |
n |
% |
HCV antibodies (+) |
90 |
2.5 |
31 |
5.1 |
16 |
1.7 |
39 |
2.0 |
1 HCV serology documented for 79% of patients (low endemicity 77%, moderate 80%, high 83%)
Table 8: HCV serological status, according to HBV* endemicity in the country of birth. Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (specialized hepatology units and hepatitis networks, France, 2008–2012) | ||||||||
Serology for Hepatitis Delta |
Total1 (N=3,173) |
Low endemicity (N=512) |
Moderate endemicity (N=786) |
High endemicity (N=1,740) |
||||
|
n |
% |
n |
% |
n |
% |
n |
% |
Anti-VHD antibodies (+) |
118 |
3.7 |
8 |
1.6 |
15 |
1.9 |
89 |
5.1 |
HDV: hepatitis delta virus,
1 documented HDV serology in 69% of patients (low endemicity 65%, moderate 68%, high 72%)
* WHO classification: HBV endemicity in the country of birth is reported for 95% of patients.
Serological status regarding HBeAg
Figure 5: Serological status regarding HBeAg. Antiviral-naive patients newly diagnosed with chronic hepatitis B (N=3,768, expert hepatology departments and hepatitis networks, France, 2008–2012)
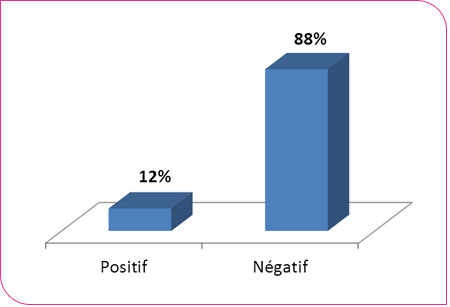
A small proportion of patients are HBeAg-positive at the time of enrollment (12%)
The proportion of HBeAg-positive patients does not differ according to the HBV* endemicity zone of the country of birth (low: 13%, medium: 11%, high: 12%)
However, among patients born in areas of high HBV* endemicity, those born in Asia are more often HBeAg-positive than those born in sub-Saharan Africa (22% vs. 10%, p < 10⁻³)
HBeAg Serology |
Total (N=3,768) |
|
|
n |
% |
Negative |
3,308 |
87.8 |
Positive |
460 |
12.2 |
Among the hepatology specialist units that participated continuously in the surveillance program between 2008 and 2012, the proportion of HBeAg-positive patients at the start of care remained stable over the period.
ALAT levels according to HBeAg serostatus
ALT levels
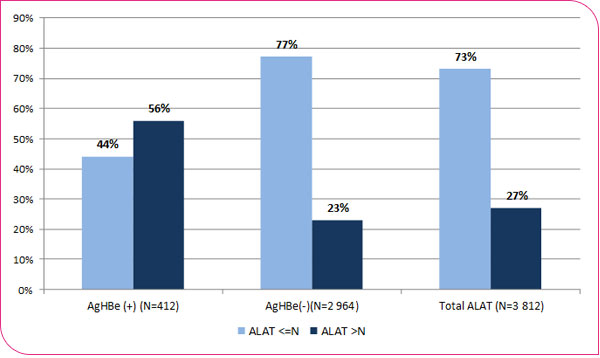
Among the 3,812 (83%) patients for whom information on ALAT levels at the start of care is available, 27% had ALAT levels above the upper limit of normal (ULN).
Among the 26 departments that participated continuously from 2008 to 2012, the proportion of patients with ALT levels above the ULN decreased, from 30% in 2008 to 21% in 2012 (p < 0.03)
HBeAg-positive patients are more likely to have ALT levels above the ULN (56%) than HBeAg-negative patients (23%) (p < 0.03)
Figure 6 - ALT levels by HBeAg status. Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (specialized hepatology units, France 2008–2012)
HBV DNA viral load by HBeAg serostatus
Figure 7 - HBV DNA viral load by HBeAg serostatus. Antiviral-naive patients newly diagnosed with chronic hepatitis B (specialized hepatology units, France, 2008–2012)
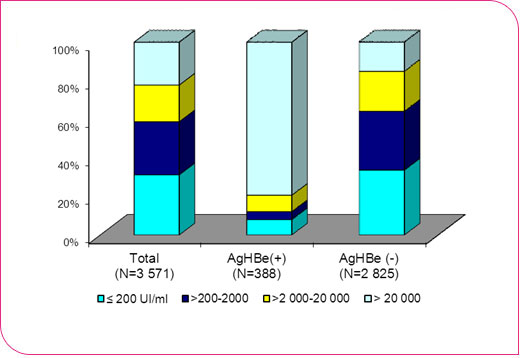
Viral load data are available for 3,571 (78%) patients: it is greater than 2,000 IU*/mL for 41% of them.
This proportion varies according to HBeAg serostatus:
36% among HBeAg-negative patients
88% among HBeAg-positive patients
* IU: International Unit/mL
HBV DNA |
Total N=3,571 |
HBeAg (+) N=388 |
HBeAg (-) N=2,825 |
|||
n |
% |
n |
% |
n |
% |
|
≤ 200 IU/mL |
1,115 |
31.2 |
31 |
8.0 |
952 |
33.7 |
200–2,000 IU/mL |
983 |
27.5 |
16 |
4.1 |
860 |
30.4 |
2,000–20,000 IU/mL |
680 |
19.0 |
33 |
8.5 |
586 |
20.7 |
20,000 IU/mL |
793 |
22.2 |
308 |
79.4 |
427 |
15.1 |
HBV genotypes
Figure 8 - Distribution of HBV genotypes. Patients who have not previously received antiviral treatment, newly diagnosed with chronic hepatitis B (N=678, specialized hepatology units, France, 2008–2012)
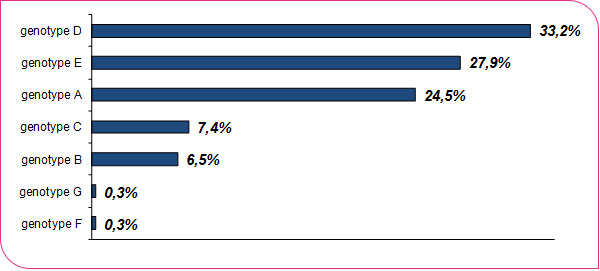
Source: National Reference Center (CNR) for Hepatitis B, C, and Delta - APHP Henri Mondor, Créteil
HBV genotyping was performed by the National Reference Center (CNR) for Hepatitis B, C, and Delta for 678 patients.
The main genotypes circulating in France are genotypes D, E, and A.
HBV genotypes according to HBV endemicity in the country of birth
Figure 9 - Distribution of HBV genotypes according to HBV endemicity* in the country of birth. Patients who had not previously received antiviral treatment and were newly diagnosed with chronic hepatitis B (N=678, specialized hepatology units, France, 2008–2012)
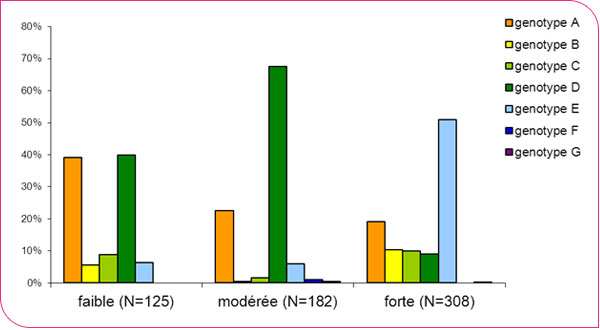
Source: National Reference Center for Hepatitis B, C, and Delta - APHP Henry Mondor, Créteil
* WHO classification
The distribution of genotypes varies according to the HBV endemicity zone of the patients’ country of birth and depends on the distribution of circulating genotypes in each of these zones.
Techniques for assessing liver fibrosis
Figure 10 - Distribution of techniques for assessing liver fibrosis used at the start of care. Patients who have not previously received antiviral treatment, newly diagnosed with chronic hepatitis B (N=2,989, expert hepatology departments, France, 2008–2012)
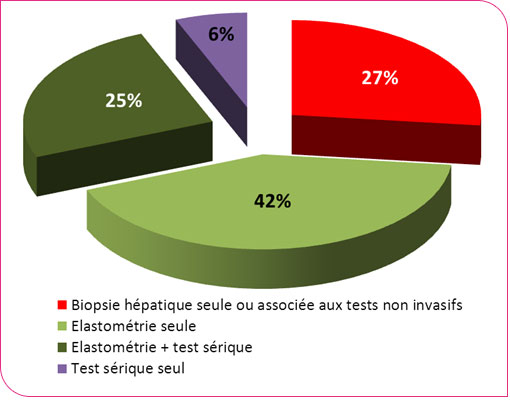
Among the 4,214 patients for whom the "fibrosis assessment" variable was recorded, nearly one-third (29%) did not undergo a fibrosis assessment at the start of care.
Among the 2,989 patients assessed at the start of care, pulse elastography was performed, either alone or in combination with another non-invasive test, in 67% of them; a liver biopsy was performed in 27%; and a serum test alone was performed in 6% of patients.
Results of Hepatic Fibrosis Assessment
Table 11: Results of liver fibrosis assessment, by technique used (biopsy or elastography). Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (specialized hepatology units and hepatitis networks, France, 2008–2012)
PBH* (N=725) |
Total n(%) |
Métavir fibrosis score | |
< F2 |
384 (53.0) |
F2 |
164 (22.6) |
F3F4 |
177 (24.4) |
Elastometry1 (N=2,008) |
Total n(%) |
≤ 9 kPa |
1,819 (90.6) |
9 kPa |
189 (9.4) |
LBP, liver biopsy, kPa, kilopascal
*LBP performed and recorded
1 Elastometry performed and reported in patients without a biopsy
Severe fibrosis (METAVIR score F3-F4) is diagnosed in 24% of patients who underwent a liver biopsy. Among patients who did not undergo a biopsy and whose fibrosis was assessed by pulse elastography, 9% had an elastography result suggestive of severe fibrosis (>9 kPa).
Severity of liver disease according to HBV endemicity, age, and sex
Figure 11 - Frequency of severe forms¹ of liver disease by age, sex, and HBV* prevalence in the country of birth. Patients who have not previously received antiviral treatment and were newly diagnosed with chronic hepatitis B (specialized hepatology units, France, 2008–2012)
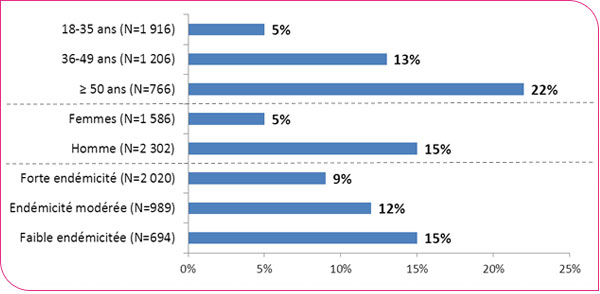
1 Severe form of liver disease defined by: a Metavir score of F3-F4 on liver biopsy and, in the absence of a biopsy, by an elastometry result > 9 kPa; and, in the absence of both biopsy and elastometry, by a clinical and histological diagnosis of cirrhosis or hepatocellular carcinoma.
*WHO classification
Among the 3,888 patients (85%) for whom an assessment of liver disease severity is available, 11% (428) had severe disease at the start of care, with this proportion remaining stable between 2008 and 2012.While patients born in countries with low or moderate HBV endemicity were more likely to have severe liver disease at the time of admission (15% and 12%, respectively) than patients born in countries with high endemicity (9%), this difference disappeared after adjusting for age.
Severity of liver damage according to alcohol consumption, HBeAg serostatus, and levels of viral load and ALT
Figure 12: Distribution of severe forms* of liver disease according to alcohol consumption, HBeAg serostatus, viral load, and ALT levels in treatment-naive patients newly diagnosed with chronic hepatitis B (specialized hepatology units, France, 2008–2012)
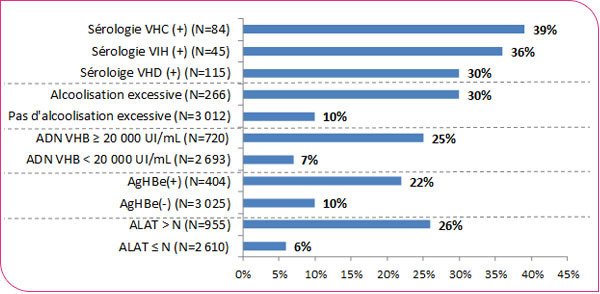
*Severe form defined as: a Metavir score of F3-F4 on liver biopsy; in the absence of a biopsy, an elastometry result > 9 kPa; and in the absence of both biopsy and elastometry, a clinical and histological diagnosis of cirrhosis or hepatocellular carcinoma.
Among the 3,429 patients for whom HBe antigen serostatus is available, severe liver disease was diagnosed in 22% of HBeAg-positive patients and in 10% of HBeAg-negative patients (p < 10⁻³).
Antiviral treatment
Figure 13 - Initiation of antiviral treatment based on the severity of liver disease, HBeAg serostatus, viral load, and ALT levels. Patients naive to antiviral therapy, newly diagnosed with chronic hepatitis B (specialized hepatology units, France, 2008–2012)
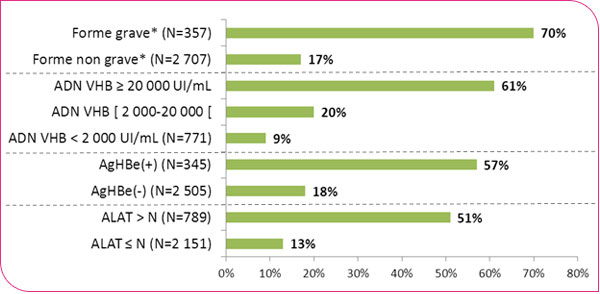
*Severe disease defined as: a Metavir score of F3-F4 on liver biopsy; in the absence of a biopsy, an elastography result > 9 kPa; and in the absence of both biopsy and elastography, a clinical and histological diagnosis of cirrhosis or hepatocellular carcinoma.
Among the 3,153 patients (69%) for whom information on the initiation of antiviral treatment is available: antiviral treatment was initiated in 23% of them, and more frequently in cases of severe liver disease, very high HBV viral load, HBeAg-positive status, or elevated ALT levels.
List of the 33 participating sites
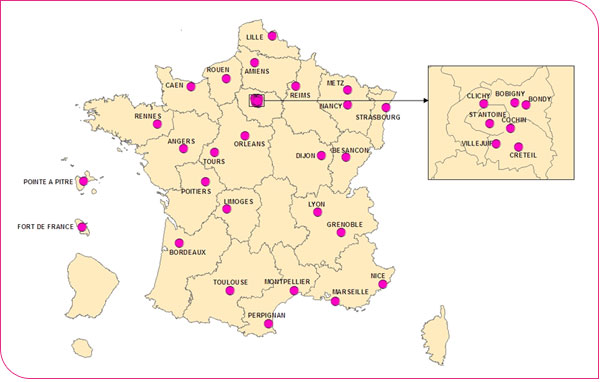
1. Alsace, New Civil Hospital of Strasbourg, Hepatobiliary-Gastroenterology Unit 2. Antilles-Guyana, Fort-de-France University Hospital, Hepatobiliary-Gastroenterology Department 3. Antilles-Guyana, Pointe-à-Pitre University Hospital, Hepatobiliary-Gastroenterology Department 4. Aquitaine Region, Bordeaux University Hospital (Haut Leveque Hospitals), Hepato-Gastroenterology Department 5. Lower Normandy Region, Caen University Hospital, Hepato-Gastroenterology Department 6. Burgundy Region, Hôpital du Bocage, Hepato-Gastroenterology Department 7. Brittany Region, Pontchaillou University Hospital, Rennes, Liver Disease Clinic 8. Centre Region, Trousseau Hospital, Tours University Hospital, Hepatogastroenterology Department 9. Centre Region, La Source Hospital, Orléans Regional Hospital, Hepatogastroenterology Department 10. Champagne-Ardenne Region, Reims University Hospital (CHU), Robert Debré Hospital, Hepato-Gastroenterology Department 11. Franche-Comté Region, Besançon University Hospital (CHU), Hepatology Department 12. Upper Normandy Region, Rouen University Hospital (CHU), Charles Nicolle Hospital, Hepato-Gastroenterology Department 13. Île-de-France Region (Paris North Network), Bichat-Beaujon University Hospital, Clichy, Hepatology Department 14. Île-de-France Region (Paris East Network), St. Antoine Hospital, Paris 12th arrondissement, Hepato-Gastroenterology Department 15. Ile-de-France Region, Creteil University Hospital (Southeast Network), Hepatogastroenterology Department 16. Ile-de-France Region (West Network), Cochin Hospital, Paris 14th arrondissement, Hepatology Department 17. Ile-de-France Region (East Network, Bondy), Jean Verdier Hospital, Hepatology Department 18. Île-de-France Region (Eastern Network, Bobigny), Avicenne Hospital, Hepatology Unit 19. Île-de-France Region (Villejuif), Paul Brousse Hospital, Hepatology Department 20. Languedoc-Roussillon Region, Montpellier University Hospital, Hepato-Gastroenterology Department 21. Languedoc-Roussillon Region, St. Jean Hospital in Perpignan, Hepato-Gastroenterology Department 22. Limousin Region, Limoges University Hospital, Gastroenterology Department 23. Lorraine Region, Metz Regional Hospital, Gastroenterology Department 24. Lorraine Region, Nancy University Hospital, Hepatogastroenterology Department 25. Midi-Pyrénées Region, Purpan University Hospital, Toulouse, Hepatogastroenterology Department 26. Nord-Pas de Calais Region, Lille University Hospital (CHRU), Gastroenterology Department 27. Eastern Pays de Loire Region, Angers University Hospital (CHU), Hepato-Gastroenterology Department 28. Picardy Region, Amiens University Hospital (CHU), Hepato-Gastroenterology Department 29. Poitou-Charentes Region, Jean Bernard Hospital, Poitiers, Hepato-Gastroenterology Department 30. PACA Region, Nice University Hospital, Hepato-Gastroenterology Department 31. PACA Region, La Conception Hospital, Marseille, Hepatology Department 32. Northern Rhône-Alpes Region, Lyon University Hospital, Hepatogastroenterology Department 33. Southern Rhône-Alpes Region, Grenoble University Hospital, Hepatogastroenterology Department
Hepatitis B worldwide according to the WHO classification