
Evaluation of the colorectal cancer screening program for the period from April 14 to December 31, 2015: National indicators
Reminder: The guaiac test (Hemoccult® II) was replaced by the immunoassay (OC Sensor®) in April 2015. This subsection presents follow-up data for individuals who participated in the program from the transition to the immunoassay through the end of 2015, specifically from April 14 to December 31, 2015.
A description of the indicators is available in the Guide to Data Formats and Definitions of Indicators for the Evaluation of the National Program
Indicators of Screening Test and Diagnostic Test Quality
This subsection presents follow-up data for individuals who participated in the program from the transition to the immunoassay test through the end of 2015, specifically from April 14 to December 31, 2015. These data cover quality indicators for screening tests and diagnostic examinations, including the rate of individuals with at least one unanalyzed test, the rate of individuals with an unanalyzed test that was not retested, the rate of positive tests, the percentage of colonoscopies performed…
The national quality indicators for screening tests and diagnostic examinations are listed in the table opposite: xls format and pdf format
Test Performance Quality
A total of 1.4 million people underwent a screening test. Among them, 79,600 (5.8%) had a test that turned out to be non-analysable. The proportion of people with an unanalyzable test was similar among men and women. This proportion increased after age 69 and was higher for a first screening than for subsequent screenings among both men and women.
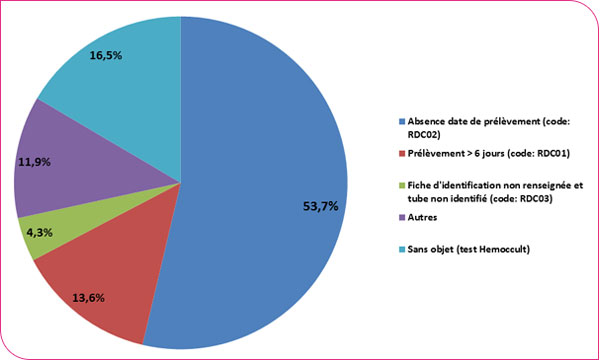
The main reasons for unanalyzable tests were: missing collection date (53.7%), submission of a sample intended for a guaiac test (16.5%), test reading deadline exceeded (i.e., more than 6 days) (13.6%), and the tube identification form left blank (4.3%).
Breakdown of reasons for non-analysis of tests
Percentage of people who underwent a colonoscopy following a positive test
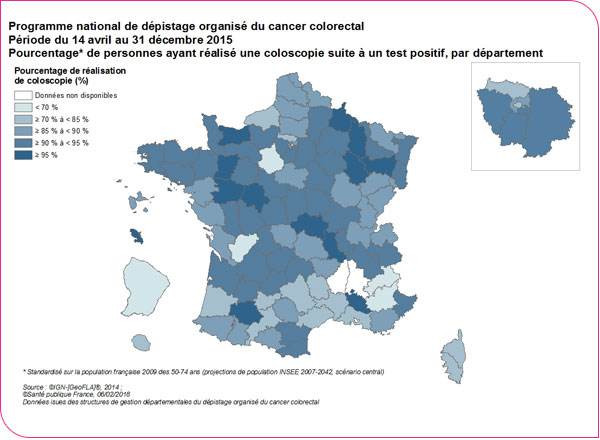
Among the 62,499 people with a positive test result, 54,875 underwent a colonoscopy, representing a colonoscopy completion rate of 88.9%. This figure is close to the recommended European benchmark (90%)1. This colonoscopy completion rate, which remained stable compared to the 2013–2014 period (88.6%), varied by department (5th percentile: 63.8%, 95th percentile: 95.8%) (Table in xls format and pdf format). Eighteen (19%) departments had rates below the acceptable European benchmark (85%).
Percentage of people who underwent a colonoscopy following a positive test
Quality of colonoscopy preparation
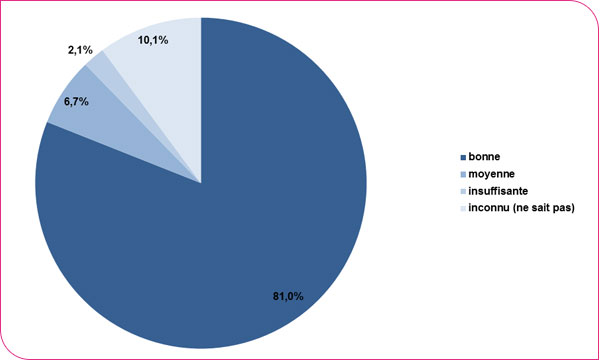
The quality of preparation for the colonoscopies performed was rated as good for 81.0%, average for 6.7%, and insufficient for 2.1% of the exams. Information on the quality of the colonoscopy was missing for 10.1% of the exams.
Distribution of colonoscopies performed by quality of preparation
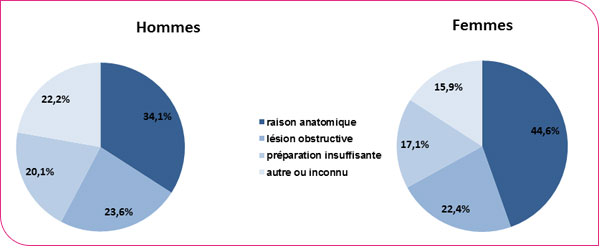
A colonoscopy is considered incomplete when the entire colon and rectum are not examined during the procedure. The percentage of people who underwent a complete colonoscopy was 92.2% (men: 92.3%, women: 92.0%). This figure is slightly higher than the acceptable benchmark recommended at the European level (90%) and lower than the desirable benchmark (95%). This figure remained stable compared to the 2013–2014 period (93.4%). The reasons why colonoscopies were incomplete varied by gender: 34.1% of cases were due to anatomical reasons among men versus 44.6% among women; 23.6% among men were due to obstructive lesions versus 22.4% among women. Other reasons included inadequate preparation (20.1% vs. 17.1%) or an unspecified reason (22.2% vs. 15.9%).
Breakdown of incomplete colonoscopies by reason
1 Segnan N, Patnick J, von Karsa L (eds). European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition. Luxembourg: European Commission, 2010.
Examination follow-up indicators
This subsection presents indicators for monitoring examinations: colonoscopy-related morbidity, the time taken to perform the colonoscopy, and the percentage of lost-to-follow-up cases among individuals who participated in the program between April 14 and December 31, 2015.
Colonoscopy morbidity
The completeness of the data collection on colonoscopy complications, particularly deaths occurring in the days following the procedure, cannot be guaranteed at the national level. In fact, for 48.8% of coloscopies, the variable recording coloscopy incidents and accidents was not filled in, meaning it is unclear whether the information is missing or whether the coloscopy proceeded without complications. Given these limitations, the statistics on coloscopy morbidity cannot be used as is.
Timeframes for Performing Colonoscopies
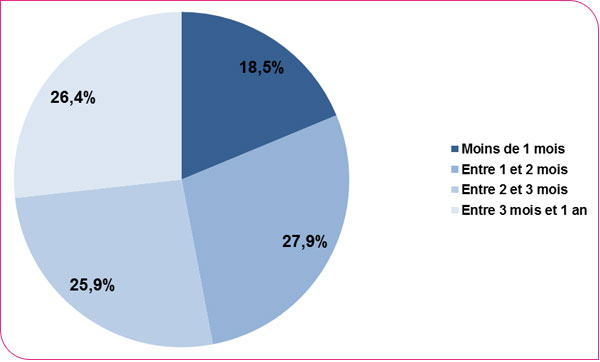
The distribution of wait times for colonoscopies following a positive test shows that only 18.5% of colonoscopies are performed within one month, in accordance with European benchmarks. The median wait time is 72 days (vs. 62 days in 2013–2014). It varies by department (5th percentile: 55.5 days, 95th percentile: 96.5 days): the shortest median wait times (< 50 days) are observed in the departments of Corsica and the Hautes-Alpes, and the longest (over 3 months: 91.3 days) in the departments of Deux-Sèvres, Haute-Loire, Haute-Saône, Maine-et-Loire, Martinique, Meuse, and Oise (Table in xls format and pdf format)
Time to completion for performed colonoscopies
Lost to follow-up
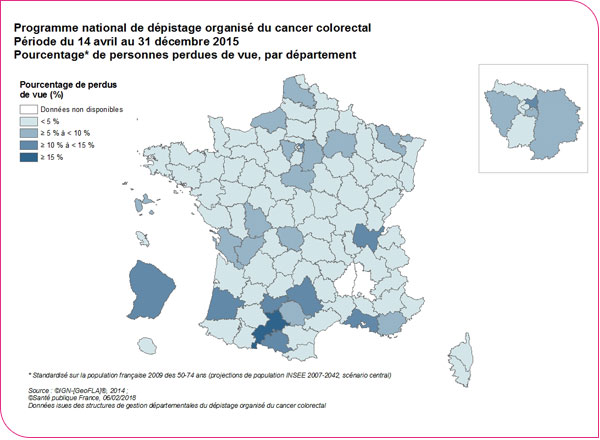
A person is considered lost to follow-up when the managing organization is unable to obtain any information about that person 24 months after the positive test result. The percentage of "lost to follow-up" cases was 3.5% (3.6% among men and 3.3% among women) for all departments participating in the program. This percentage varied by department: from 1.5% at the 5th percentile to 6.0% at the 95th percentile (Table in XLS and PDF formats). These departmental disparities reflect the heterogeneity of documentation within the management structures and test follow-up systems (for example, the transmission of information by healthcare professionals to the management structure is more or less systematic).
Geographic distribution of the percentages of lost-to-follow-up cases
Indicators of detected lesions
This subsection presents indicators of lesions detected in individuals who participated in the program between April 14 and December 31, 2015. These indicators relate to the nature and rates of lesions detected (adenomas, advanced adenomas, and cancers) through diagnostic examinations (colonoscopy or other).
During this 8.5-month invitation period, the program detected nearly 21,300 advanced neoplastic lesions (16,974 advanced adenomas and 4,279 colorectal cancers), compared to 20,900 over a period of nearly 24 months in 2013–2014.
The detection rate for advanced adenomas (or colorectal cancers) is defined as the proportion of patients in whom an advanced adenoma (or cancer) is the most serious lesion detected, among those who underwent an analyzable screening test. It is expressed per 1,000 (‰) screened individuals.
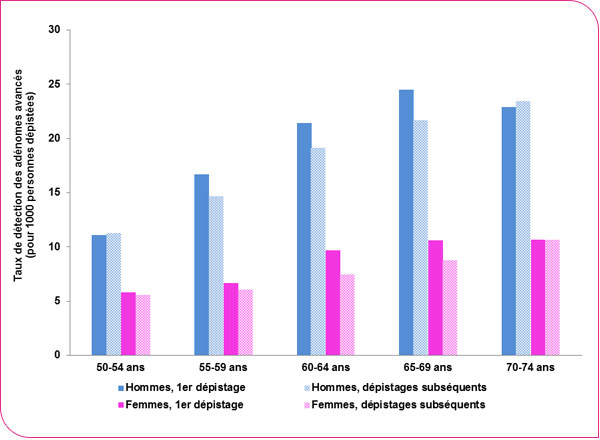
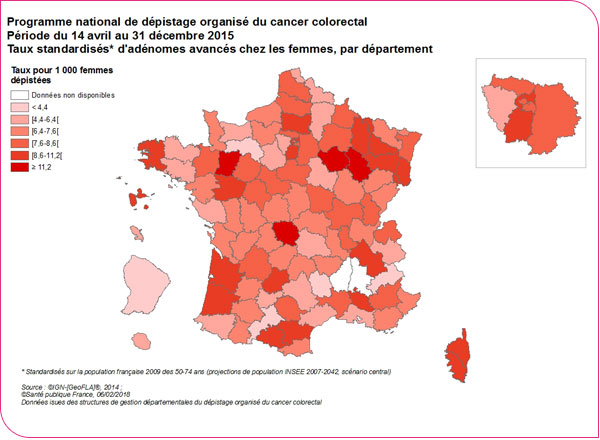
The detection rate for advanced adenomas (adenomas 10 mm or larger, or with high-grade dysplasia, or a villous component) was 12.1 per 1,000 screened individuals (Table in xls format and pdf format).
The detection rate for advanced adenomas was higher among men than among women; it increased with age and was higher during the first screening than during subsequent screenings (see figures below).
Distribution of the detection rate for advanced adenomas by age, sex, and screening round (adenoma 10 mm or larger, or with high-grade dysplasia, or villous component)
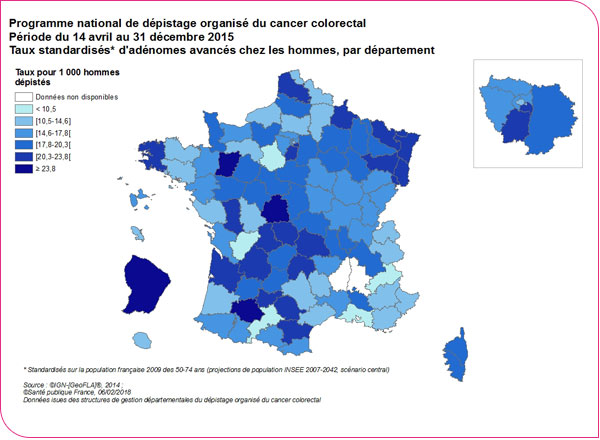
The detection rate of advanced adenomas (adenomas 10 mm or larger, or with high-grade dysplasia, or a villous component) varied by department: from 10.4‰ at the 5th percentile to 23.7‰ at the 95th percentile among men and from 4.3‰ at the 5th percentile to 11.1‰ at the 95th percentile among women (Table in xls format and pdf format).
Detection rate of advanced adenomas for men
Detection rate of advanced adenomas for women
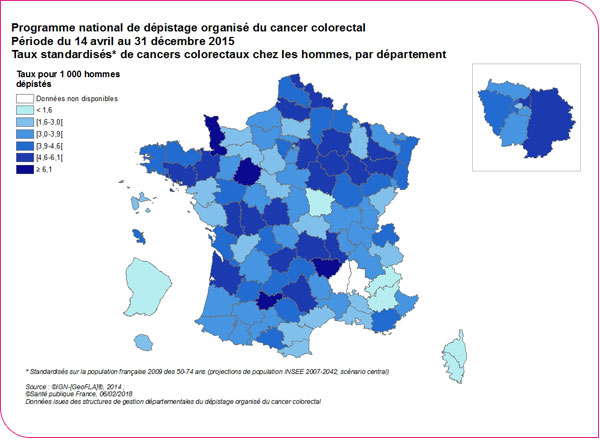
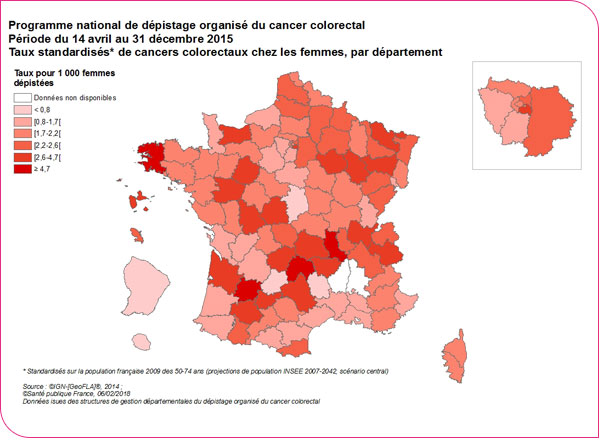
The cancer detection rate was 2.9 per 1,000 people screened. It varied by age, sex, and screening round. For women, it is 2.0‰ during the first screening and 2.3‰ during subsequent screenings, whereas for men, it is 4.0‰ and 4.4‰, respectively—twice as high (Table in XLS and PDF formats). It also varies by department: from 1.5‰ at the 5th percentile to 6‰ at the 95th percentile for men, and from 0.7‰ at the 5th percentile to 4.6‰ at the 95th percentile for women (Table in XLS and PDF formats).
Colorectal cancer detection rates for men
Colorectal cancer detection rates for women
Detection rates for advanced adenomas and colorectal cancers depend heavily on the departmental incidence of cancer and the performance of departmental programs in detecting these lesions. Indeed, the percentage of eligible individuals who undergo a colonoscopy following a positive test result and the percentage of individuals for whom the managing facility lacks a final diagnosis (lost to follow-up or final diagnoses unknown) are factors that influence the recording of these lesions and may help explain departmental disparities. Furthermore, as defined in the "Guide to Data Format and Definitions of National Program Evaluation Indicators," advanced adenomas are adenomas 10 mm or larger in size, with villous or tubulo-villous components, or with high-grade dysplasia. The lack of intra- and inter-examiner reproducibility in the diagnosis of advanced adenomas may also help explain the departmental differences in observed advanced adenoma rates[1].
[1] Denis, B., Bottlaender, J., Breysacher, G., Chiappa, P., Peter, A., Weiss, A.-M. The advanced adenoma: A topical concept but an out-of-date definition? (2011) Hepato-Gastro, 18 (3), pp. 269-276.
Stages of detected cancers
The stage of cancers detected by the organized screening program was determined according to the international TNM classification of malignant tumors¹. This classification allows cancers to be categorized based on their degree of anatomical spread: local (or T), lymph node (or N), and metastatic (or M) involvement. As it applies, for the colon and rectum, only to adenocarcinomas, these are described in this section. For colon cancers, the pTNM histopathological classification was used. For rectal cancers, which may undergo neoadjuvant therapy prior to surgery—resulting in a change in the T, N, or M stage of the detected tumor—the quality of available data and the heterogeneity of methods for documenting staging information do not allow for the determination of the TNM stage prior to treatment. Consequently, only colon cancers (including the rectosigmoid junction) and rectal cancers that did not receive neoadjuvant therapy were included.
The cancer stage is considered unknown when at least one of the T, N, or M data points is unknown (unless pT=Tis, in which case the TNM stage is in situ, or if M=M1, in which case the TNM stage is IV). Among the adenocarcinomas of the rectum (without neoadjuvant treatment) and colon detected, this information is missing in 34.6% of cases. When the stage cannot be determined, T is missing in 20.3% of cases, N is missing in 23.2% of cases, and M is missing in 33.8% of cases. This percentage of adenocarcinomas of unknown stage reflects significant regional variation: it ranges from 0% to 100% (Table in XLS and PDF formats), as information on the metastatic status of detected cancers is difficult to access.
The description covers only the 41 departments with less than 30% missing data on cancer stages, corresponding to 2,048 detected colorectal adenocarcinomas (without neoadjuvant treatments). Among these adenocarcinomas, 8.5% are of unknown pTNM stage.
Among adenocarcinomas with known stages, 32.1% are carcinomas in situ and 67.9% are invasive cancers (stages I to IV), of which 46.1% are stage I, 21.5% are stage II, 21.9% are stage III, and 10.1% are stage IV (Table in xls format and pdf format).