
Rubella: 2012 Epidemiological Data
In 2012, the Rénarub network comprised 194 laboratories nationwide, including 185 in metropolitan France and 9 in the overseas departments. The effective participation rate of the laboratories contacted was 85% (laboratories participating in both survey semesters), with 99% of laboratories participating in at least one survey semester (see list of participating laboratories). The return rate for files sent to clinicians was 95% (142 out of 149 files).Twelve confirmed maternal rubella primary infections and one probable reinfection were identified in mainland France, none in the overseas departments and territories (Table 1). Three congenital infections were diagnosed, but no congenital rubella-associated malformations were identified.
Table 1 – Distribution of the number of cases reported in mainland France according to case definitions | ||||||||
|
2005 |
2006 |
2007 |
2008 |
2009 |
2010 |
2011 |
2012 |
Number of cases reported by laboratories (IgM+) |
110 |
118 |
75 |
65 |
144 |
123 |
140 |
149 |
Excluded cases |
94 |
111 |
70 |
63 |
137 |
119 |
132 |
136 |
Possible primary or reinfection |
5 |
7 |
4 |
7 |
14 |
6 |
5 |
6 |
Lost track of, files not returned |
9 |
26 |
4 |
31 |
47 |
23 |
12 |
17 |
Absence of pregnancy |
22 |
11 |
22 |
9 |
17 |
15 |
20 |
36 |
Rubella immunity prior to pregnancy |
55 |
65 |
40 |
16 |
52 |
69 |
83 |
61 |
Other (including vaccination during pregnancy) |
3 |
2 |
7 |
6 |
12 |
16 |
||
Confirmed and probable maternal rubella infections |
16 |
7 |
5 |
2 |
7 |
4 |
8 |
13 |
Confirmed primary infections |
11(*) |
3 |
4 |
1 |
5 |
2 |
5 |
12 |
Confirmed reinfections |
1 |
|||||||
Confirmed infections |
1 |
|||||||
Probable primary infections |
2 |
2 |
1 |
1 |
1 |
3 |
||
Probable re-infections |
1 |
1 |
1 |
1 |
1 |
1 |
||
Probable infections |
1 |
|||||||
|
|
|
|
|
|
|
||
Number of congenital infections |
9 |
0 |
2 |
0 |
2 |
1 |
2 |
3 |
Congenital rubella syndrome (newborns) |
2 |
1 |
1 |
|||||
Rubella with congenital malformations (pregnancy termination) |
1 |
|||||||
Non-teratogenic rubella infection or unknown clinical status (newborns or fetuses) |
7 |
2 |
1 |
1 |
3 |
|||
(*) twin pregnancy
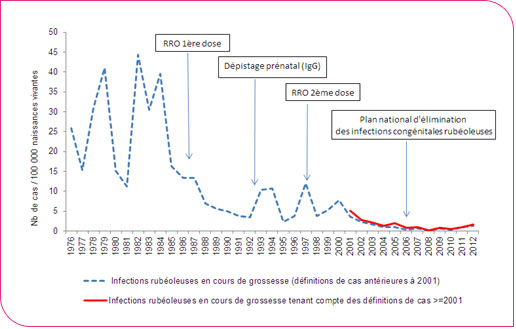
In 2012, the ratio of "rubella infections during pregnancy recorded by Rénarub / number of live births (LB)" in mainland France was 1.64 per 100,000 in 2012 (Figure 1). This is the highest ratio observed since 2005.
Trend in the ratio of rubella infections in pregnant women to live births – Metropolitan France, 1976–2012 (MMR = trivalent measles-mumps-rubella vaccine)
The pregnancy outcome was reported for 12 of the 13 cases. Among the 8 children born to infected mothers, 1 was born infected and showed signs of fetal pathology without abnormalities suggestive of congenital rubella syndrome, 5 were born uninfected, and for 2 asymptomatic children, the infection status was not determined. Three pregnancies were terminated (medically or spontaneously). In another pregnancy, fetal infection was ruled out in the stillborn child.
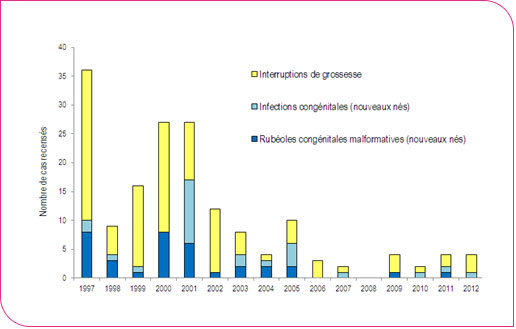
Trend in the number of maternal infections leading to pregnancy terminations or the birth of children with congenital rubella syndrome – 1997 to 2012
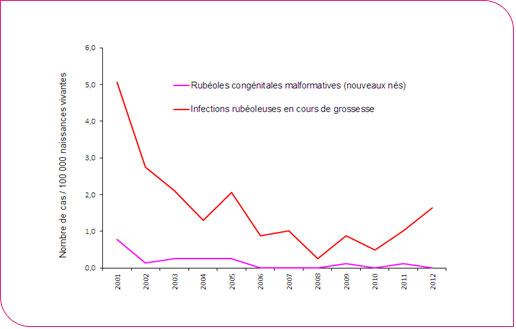
The ratio of "newborns with congenital rubella syndrome (CRS) recorded by Rénarub / number of live births (LB)" in mainland France was zero.
Trends in the ratio of rubella infections in pregnant women to cases of congenital rubella syndrome among live births – Metropolitan France, 2001–2012
Among the 13 maternal infections, the mother’s country of birth was documented for 9 of them, and 6 were born outside France (North Africa, West Africa, and Eastern Europe).While between 2003 and 2006, the "infections per live births" rate was higher among young women aged 15–19 (13.1 to 20.1 cases per 100,000 live births depending on the year), this rate has been zero for this age group since 2008 (Table 2). In contrast, these ratios were highest among women aged 20–24 and 25–29.
Table 2 - Rubella infection rates by age of pregnant women by year, mainland France, 2003–2012 | |||||||
Ratio of infections per 100,000 live births |
|||||||
Age groups |
Average 2003–2006 |
2007 |
2008 |
2009 |
2010 |
2011 |
2012 |
15–19 years |
11.8 |
6.8 |
0.0 |
0.0 |
0.0 |
0.0 |
0.0 |
20–24 years |
5.6 |
2.9 |
0.0 |
0.0 |
1.0 |
1.9 |
3.0 |
25–29 years |
0.6 |
0.0 |
0.4 |
1.2 |
0.4 |
1.6 |
2.9 |
30–34 years |
0.6 |
0.4 |
0.0 |
0.8 |
0.4 |
0.8 |
0.7 |
35–39 years |
0.4 |
0.0 |
0.0 |
0.7 |
0.0 |
0.0 |
0.8 |
40–44 years old |
1.8 |
0.0 |
3.2 |
3.1 |
3.1 |
0.0 |
0.0 |
Total |
1.5 |
0.6 |
0.1 |
0.9 |
0.5 |
1.0 |
1.6 |
The 13 maternal infections in 2012 occurred in 5 regions (Table 3). The Languedoc-Roussillon region was the most affected, with an infection rate of 13.0 per 100,000 live births.
Table 3 – Rubella infection rates by age of pregnant women by year, mainland France, 2012 | ||
Region |
Number of cases |
Ratio of infections per 100,000 live births |
Brittany |
1 |
2.7 |
Ile-de-France |
6 |
3.3 |
Languedoc-Roussillon |
4 |
13.0 |
PACA |
1 |
1.7 |
Poitou-Charentes |
1 |
5.4 |
Mainland France |
13 |
1.6 |
Data collected through the Rénarub network in 2012 continue to indicate low residual circulation of the rubella virus, reflecting a high level of immunity among women of childbearing age due to catch-up vaccination.
This level of susceptibility to the virus was estimated at 4% among women aged 20–29 and 5% among women aged 30–39 in the seroprevalence survey conducted in 2009–2010 in mainland France1. However, the level of susceptibility is higher among men (13% among those aged 20–29), and vaccination coverage rates in France vary by department,2 which could facilitate the emergence of localized outbreaks of viral circulation.
Nearly half of maternal infections in 2012 involved women born in countries where vaccination programs do not include rubella vaccination.
The actual number of maternal infections may be underestimated within the Rénarub network, primarily due to a lack of diagnosis in pregnant women, as rubella infections are frequently asymptomatic or atypical.
The active participation, since Rénarub’s creation, of specialized laboratories—which receive control samples when a maternal infection is suspected—suggests that even if the network is not entirely comprehensive, and even if the participation rate of all laboratories or clinicians is not 100%, the vast majority of confirmed and probable cases are captured by the surveillance system.
The National Reference Center (NRC) for Materno-Fetal Rubella Infections was established in 2012 to provide expertise to laboratories, diagnostic support when needed, assistance in dating maternal primary infections, and to contribute to epidemiological and virological surveillance.
The NRC is now integrated into the data transmission system for data collected by partner laboratories in the Rénarub network.